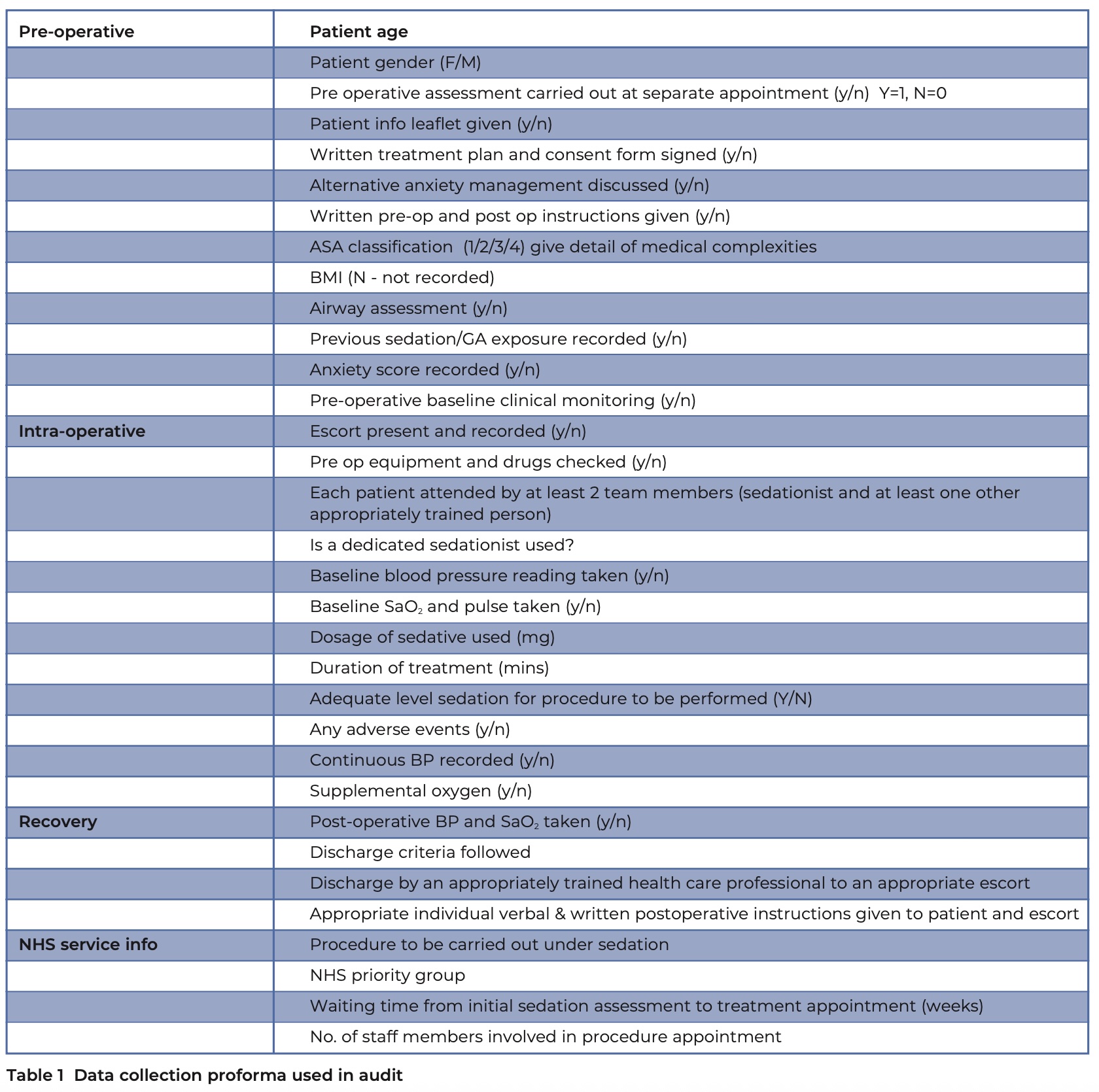
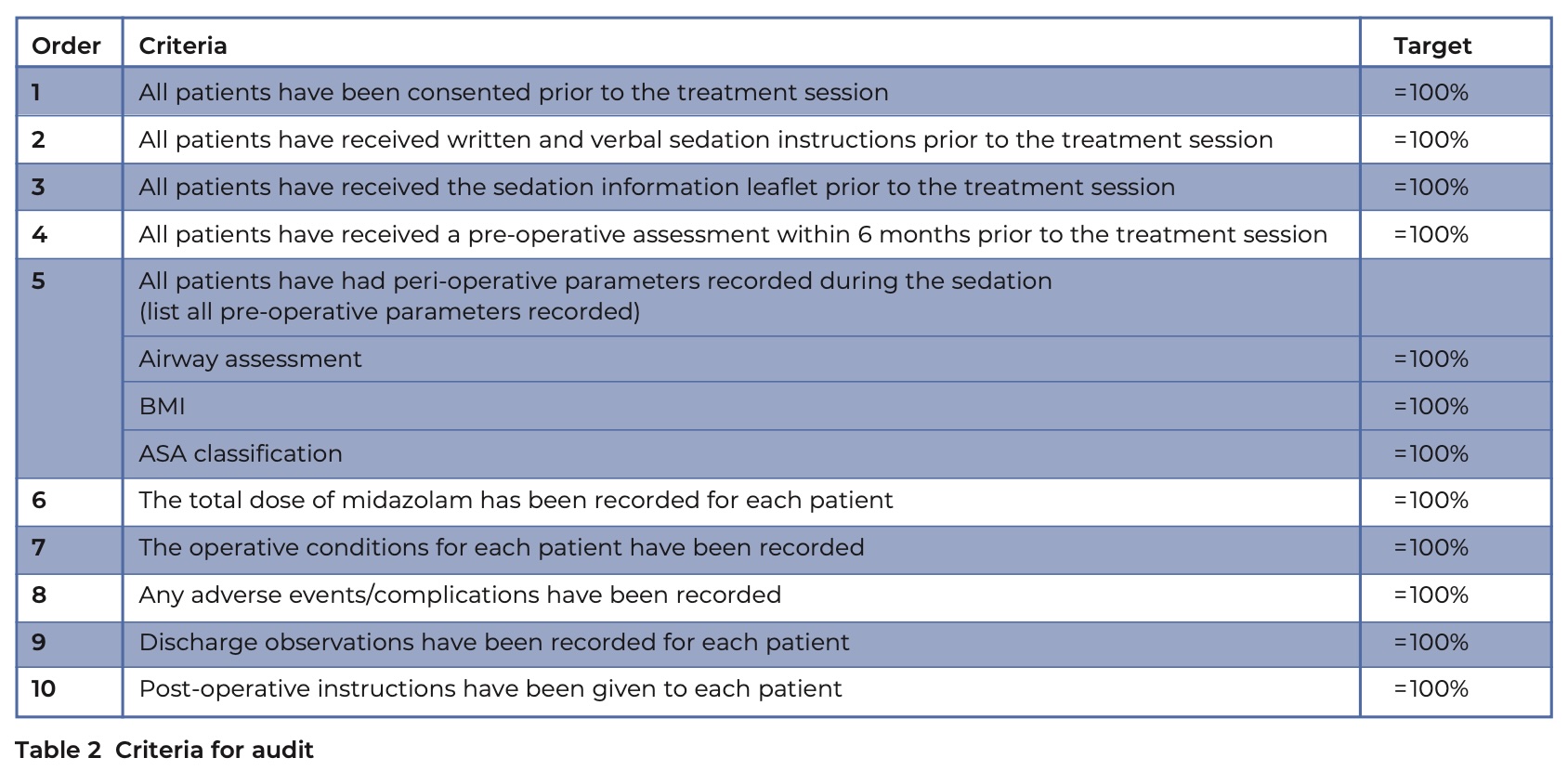
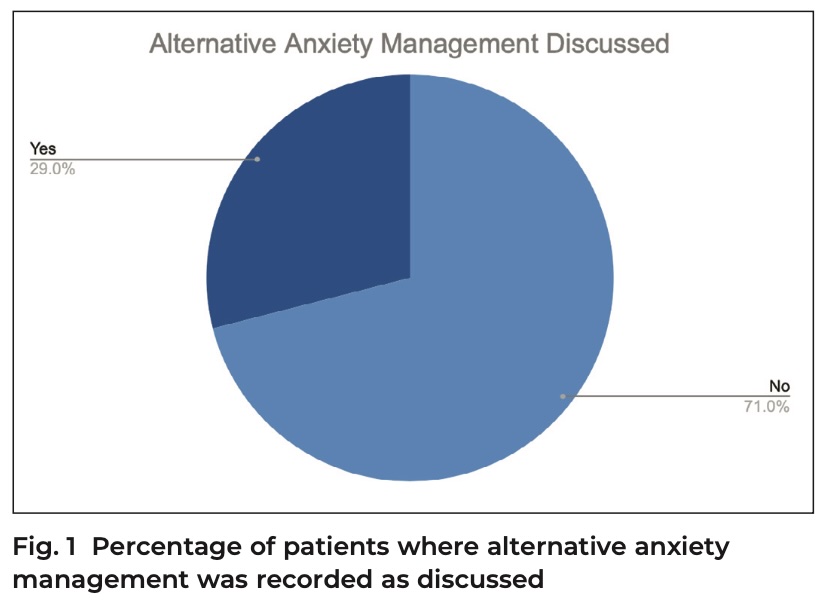
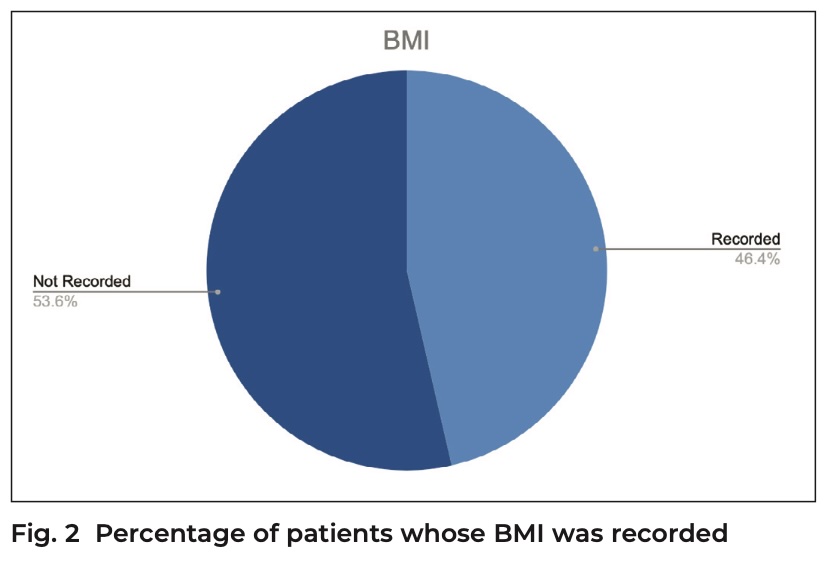
Please click on the tables and figures to enlarge
The combined use of oral / transmucosal midazolam sedation with IV remimazolam for special care patients – a case series
N. Storch*1 BDS
M. Doshi2 BDS (Hons) MSc (Spcsed)
1Dental Core Trainee, East Surrey Hospital, Canada Avenue, RH1 5RH
2Consultant in Special Care Dentistry, East Surrey Hospital, Canada Avenue, RH1 5RH
*Correspondence to: N. Storch
Email: nicola.storch@nhs.net
DOI: 10.63507/RHEB8576
Abstract
Introduction
Remimazolam, a short-acting benzodiazepine, is increasingly being used for dental sedation in the UK. Current guidance from the Intercollegiate Advisory Committee on Sedation in Dentistry advises that remimazolam and midazolam should not be used together routinely. At the time of writing, no published literature described the combined use of oral / transmucosal midazolam with intravenous remimazolam.
Case series
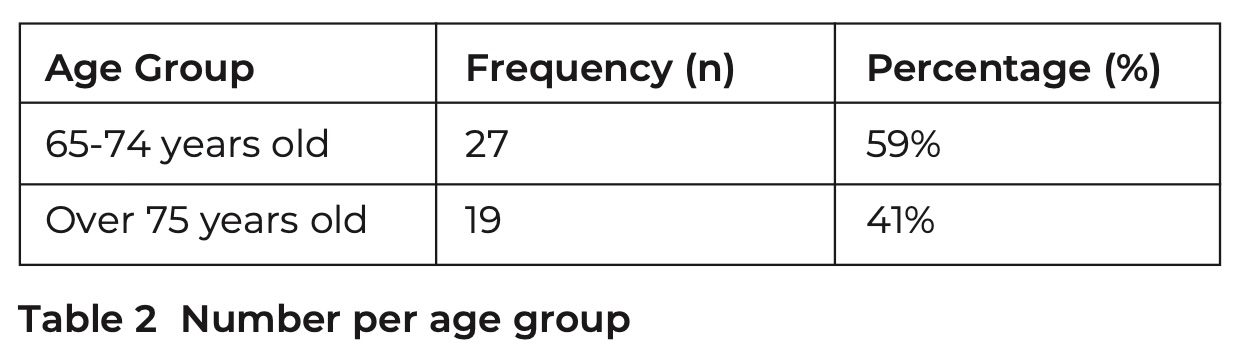
This paper presents a series of cases in which midazolam pre-medication was followed by intravenous remimazolam to support patients in special care undergoing dental treatment. Pre-medication ranged from 10 to 20 mg of midazolam and included both intranasal and oral forms. Patient factors influencing the choice to use remimazolam included an increased risk of respiratory depression, dysphagia, the previous need for flumazenil, and patient age.
Outcomes
In all cases, recovery was uneventful with no need for supplemental oxygen or use of flumazenil. Recovery times ranged from 25 to 57 minutes. The combined use of midazolam and remimazolam is beneficial in patients where a faster return to baseline is desired.
Key learning points
- At present, no literature describes the combined use of oral / transmucosal midazolam and intravenous remimazolam for dental procedures
- In this case series, treatment was completed successfully with no adverse events
- More evidence is needed to assess the synergistic effects of these two drugs to justify the combined use.
Introduction
Conscious sedation is a well-established technique that enables the safe and effective delivery of dental care for patients with special needs, including those with learning disabilities, autism and dementia. In some cases, these patients cannot tolerate the placement of a cannula, and adjunctive methods may be required. These methods can include planned clinical holding by trained staff, topical local anaesthesia, inhalation sedation with nitrous oxide, or oral or transmucosal midazolam to facilitate safe cannulation. Transmucosal or oral sedation with midazolam, often followed by intravenous (IV) midazolam, has been successfully used in special care dentistry for many years, significantly improving access to a range of dental treatments for these patient groups.1
Remimazolam, a short-acting benzodiazepine, is increasingly being used for dental sedation in the UK across all areas. Its rapid onset and metabolism offer potential advantages, particularly in special care dentistry, where a fast uptake and quicker recovery to baseline may enhance patient experience and safety.2, 3 The Intercollegiate Advisory Committee on Sedation in Dentistry (IACSD) issued interim guidance in 2022, advising that remimazolam and midazolam should not be used together routinely or without clear justification in primary care settings.4 At the time of writing, no published literature describes the combined use of midazolam pre-medication with IV remimazolam.
For over 30 years, midazolam has been an effective and safe drug for conscious sedation in special care dentistry. However, one disadvantage of midazolam is its variable recovery time.5 Even with an excellent safety record in dentistry and generally low incidence of complications in dental settings, all benzodiazepines carry a risk of respiratory depression, particularly at higher doses.6 The metabolism and excretion of midazolam can be significantly prolonged in older patients or those with impaired hepatic or renal function, which increases recovery times.7
IV remimazolam offers several clinical advantages over midazolam, the most notable being its significantly faster recovery time, typically ranging from 10 to 40 minutes, compared to 20 to 80 minutes with midazolam.8 It also has a more rapid onset of action, occurring within one to two minutes, compared to approximately three minutes for midazolam.9 Remimazolam demonstrates a much shorter half- life of around 0.75 hours,9 and has nearly three times the elimination clearance of midazolam, owing to its metabolism by tissue esterases rather than hepatic pathways.8 This pharmacokinetic profile contributes to its more predictable and rapid clearance, which is particularly important in patients with hepatic or renal impairment. These properties make remimazolam particularly well suited for use in short dental procedures where a quick return to cognitive and motor baseline is desirable, as well as in patient groups where prolonged recovery may pose additional risks, such as older adults, medically compromised individuals, or those with a history of delayed prolonged sedation with midazolam.
Midazolam is frequently used as a pre-medication in various forms. Transmucosal midazolam has a rapid onset and reaches a maximum concentration around 10 to 14 minutes. In contrast, the oral form takes 15 minutes or longer, resulting from lower bio-availability due to extensive first-pass metabolism.7 Both remimazolam and midazolam enhance GABA activity; however, there are no specific studies on their potential interactions. Concomitant benzodiazepines may result in higher plasma concentrations and have an increased risk of toxicity. However, this is based on competition for the same substrates during metabolism.8, 10 Remimazolam and midazolam are metabolised by different enzymes, which may counteract this risk.
The oral bio-availability of remimazolam is negligible, rendering it unsuitable for oral premedication. Limited studies are available on the use of intranasal remimazolam, which reduced pre-operative anxiety in children,11 but has been associated with nasal discomfort.12
Combining oral or nasal midazolam with IV remimazolam may lead to a reduction in overall recovery time. However, due to pharmacokinetics, remimazolam is likely to wear off before midazolam.
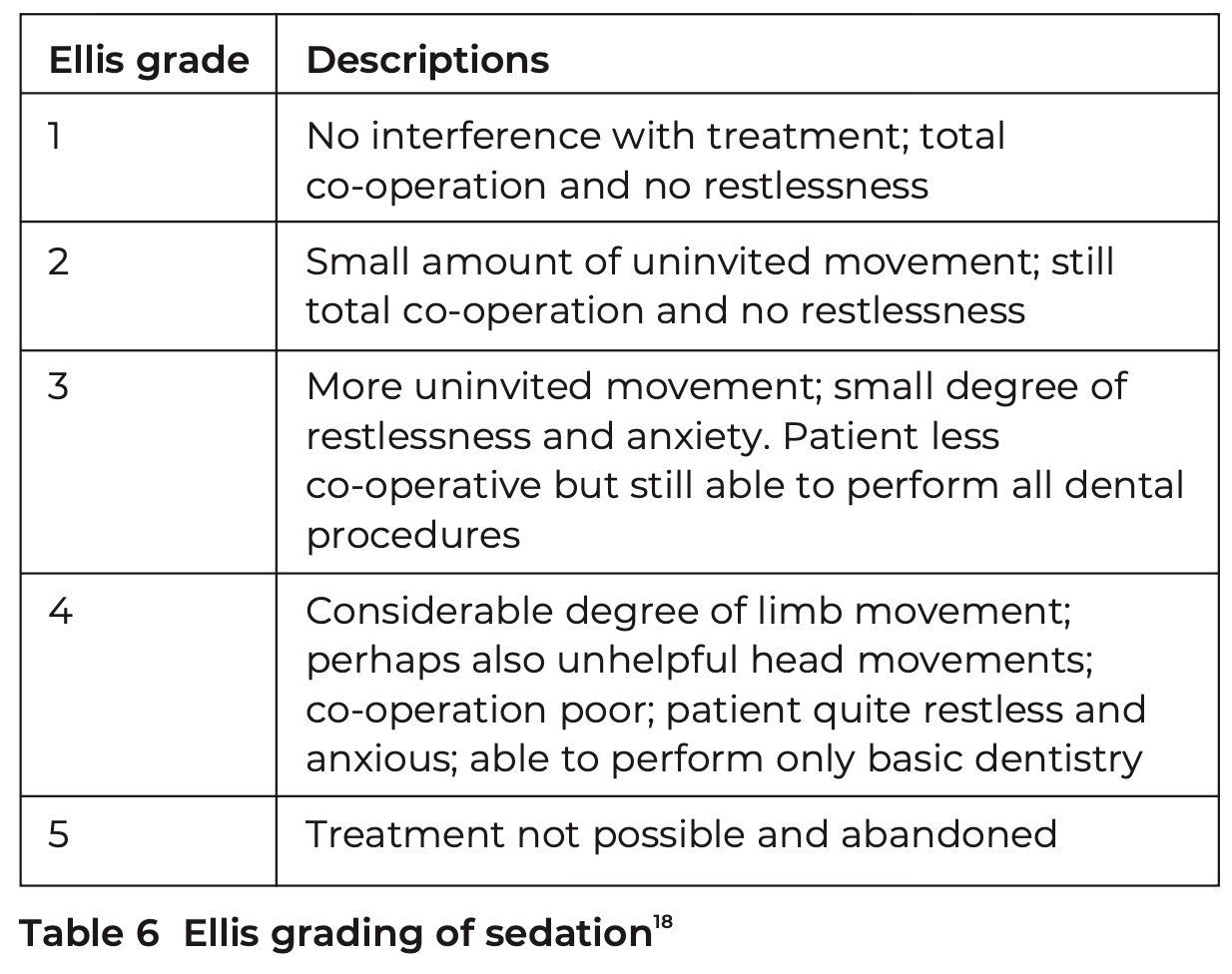
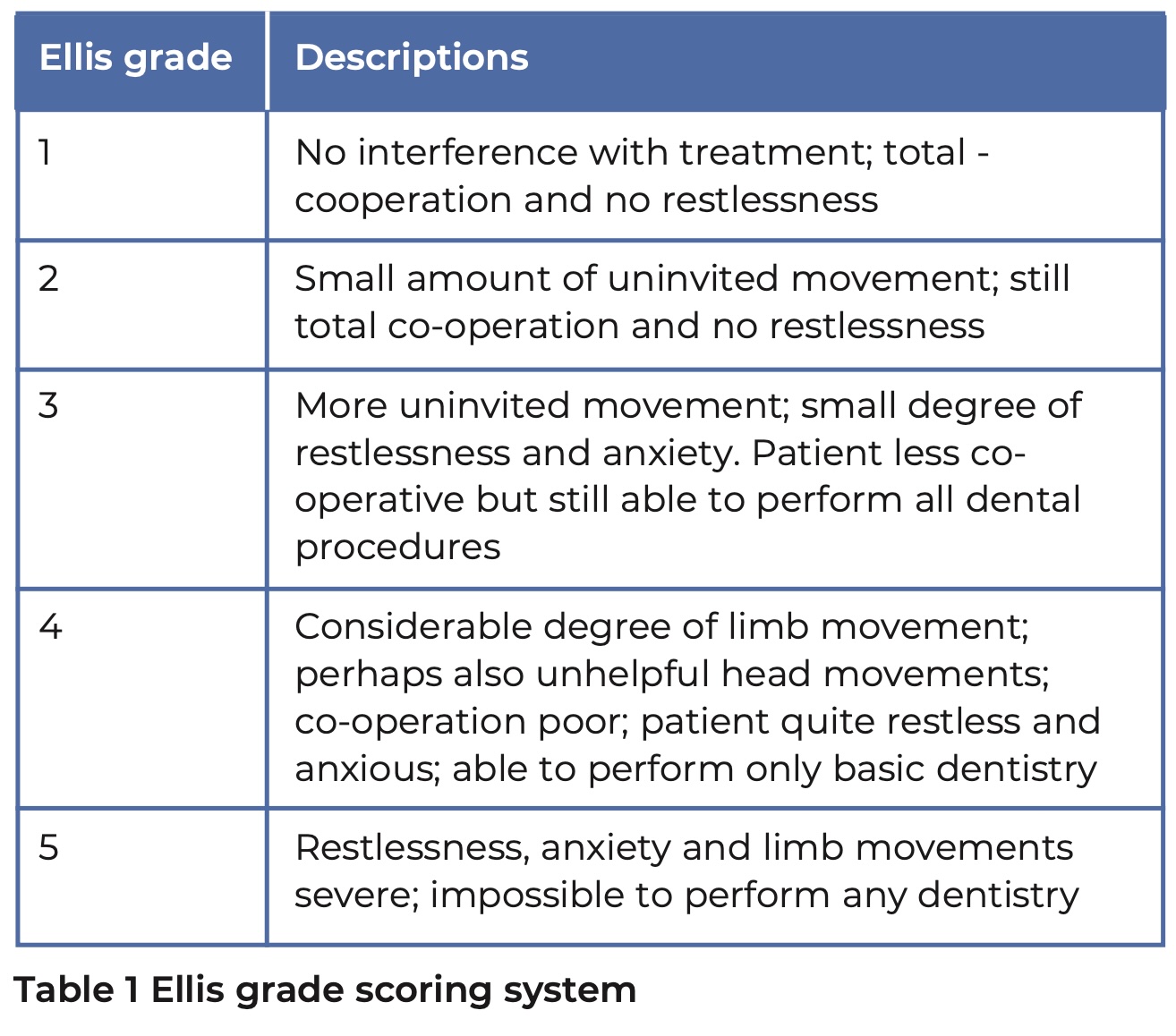
This paper presents a series of cases in the Special Care Dental Service at Surrey and Sussex Health Care NHS Trust where midazolam pre-medication was followed by IV remimazolam, illustrating how this approach can facilitate faster recovery, particularly when initial sedation is administered via oral or transmucosal routes. The team at Surrey and Sussex Healthcare NHS Trust is experienced in sedation and based on early clinical use of remimazolam, has adjusted the starting dose from the manufacturer's recommended guidelines of 7 mg to 5 mg as standard, and from 5 mg to 3 mg for older and more medically complex patients, with maintenance increments of 1 to 2 mg at a minimum interval of 2 minutes.13 Treatment was carried out in a dental clinic setting with a dentist providing the sedation and the Ellis grade scoring system was used to assess co-operation (Table 1).14
Case 1 – a patient with Down’s syndrome
A 58-year-old patient with Down’s syndrome attended the special care dentistry department for radiographic examination and treatment of carious teeth under sedation. Medically, the American Society of Anaesthesiologists grading (ASA) was 3 with a severe learning disability, autism, anxiety and well-controlled epilepsy. Previously, he had been seen on a domiciliary visit where only a limited examination revealed multiple carious lesions. There were concerns from his carers that he was in pain.
This patient had a short neck with excess soft tissue, which contributed to airway considerations; therefore, remimazolam was chosen for finer control over sedation levels.
Pre-operative observations were not possible due to a lack of co-operation, and the patient had a history of challenging behaviour, being unable to accept blood tests. Subsequently, a 20 mg oral midazolam was administered, allowing for the successful cannulation and titration of 7 mg (in increments of 3 mg, 2 mg, and 2 mg) of IV remimazolam over 10 minutes. The completed treatment included an examination, radiographs, and the extraction of three grossly carious teeth, along with blood test samples for his general practitioner. During the procedure, oxygen saturation levels dropped below 90%, which was effectively managed with an airway manoeuvre (head tilt, chin lift). There was an uneventful recovery, and the patient was discharged 57 minutes after the last dose of remimazolam was provided.
Case 2 – previous midazolam sedation requiring flumazenil
A 34-year-old patient with a severe learning disability and autism attended for examination under sedation. He had an ASA classification of 2 and was otherwise fit and well. Due to his behaviour, it was not possible to undertake any form of oral assessment. He underwent an examination under sedation with nasal and IV midazolam five years ago, during which he required full mouth debridement and no additional dental procedures. Recovery has been challenging as he wanted to get up and leave before the effects of the midazolam had worn off, posing a risk of falling and injuring himself, resulting in 500 micrograms of flumazenil being administered to support a safer recovery.
Since then, no examinations have been possible due to limited co-operation, and the patient has found it increasingly difficult to leave his home following the COVID-19 pandemic. Sedation was chosen over a general anaesthetic as treatment needs had been low in the past. Remimazolam was selected for the faster recovery, given the sedation history.
To facilitate cannulation, 20 mg of oral midazolam was administered, followed by 16 mg of remimazolam titrated over 12 minutes. Sedation scoring was 3, and the Ellis grade was 3, with movement and a strong bite hindering the obtaining of diagnostic radiographs. Nevertheless, a comprehensive examination and a glass ionomer restoration of a carious third molar were performed. Blood test samples were collected as required by his general medical practitioner to evaluate his overall health. Recovery was uneventful, and he was discharged 39 minutes later. A decision was made that anaesthetist-led sedation or general anaesthesia would be necessary in the future to facilitate full-mouth radiographs and to assess the quality of the restoration placed.
Case 3 – a patient with severe dysphagia and aspiration risk
A 43-year-old patient attended for treatment under sedation. She had Cri du Chat syndrome, severe learning disability, and dysphagia, resulting in an ASA of 2. She had experienced multiple episodes of sedation, on average every two years, requiring debridement and extraction of teeth due to periodontal disease. Her carers found it very challenging to undertake oral care due to tight oral musculature and care- resistant behaviour. A limited examination was possible, revealing extensive calculus and gingivitis.
Remimazolam was selected because only a brief period of sedation was necessary. The patient’s dysphagia made greater control over the sedation duration and a quicker return to baseline desirable to minimise the aspiration of oral secretions during recovery.
As a premedication, 10 mg of intranasal midazolam was administered, followed by 13 mg of remimazolam over 20 minutes. The sedation score was 3, and the Ellis grade was 3. Excessive movement and gagging prevented acceptable intraoral radiographs but permitted thorough full-mouth debridement. Blood test samples were taken again. Recovery was uneventful, and she was discharged 37 minutes after the last dose of sedation.
Case 4 – an older patient requiring dental extractions
A 71-year-old patient attended for dental extractions of mobile anterior teeth that were causing him pain. Medically, he had a severe learning disability, hypothyroidism, fatty liver disease and agoraphobia with an ASA of 3. Existing co-operation was limited, with only a very brief examination possible.
Initially, oral sedation was not planned since cannulation had been successful in previous IV sedation procedures. However, the patient became upset during cannulation and left the room. At this point, 10 mg of oral midazolam was administered; a reduced dose was used due to the patient’s age. The baseline saturation dropped from 96% to 94% before successful cannulation, and IV remimazolam was chosen due to the anticipated short duration. Older patients also have a higher risk of prolonged recovery and falls, so a faster recovery time is desirable.
Only 2 mg of remimazolam was needed, allowing the successful clearance of the two remaining mobile anterior teeth with a five minute surgery time. Recovery was uneventful, and the patient was discharged 25 minutes later.
Discussion
These four cases demonstrate that combining IV remimazolam with with oral / transmucosal midazolam is a potentially effective technique that benefits special care patients for various reasons. A summary is presented in Table 2. All cases were performed by a consultant in special care dentistry who has previously treated three of these patients under sedation with midazolam and reported a smoother and faster recovery.
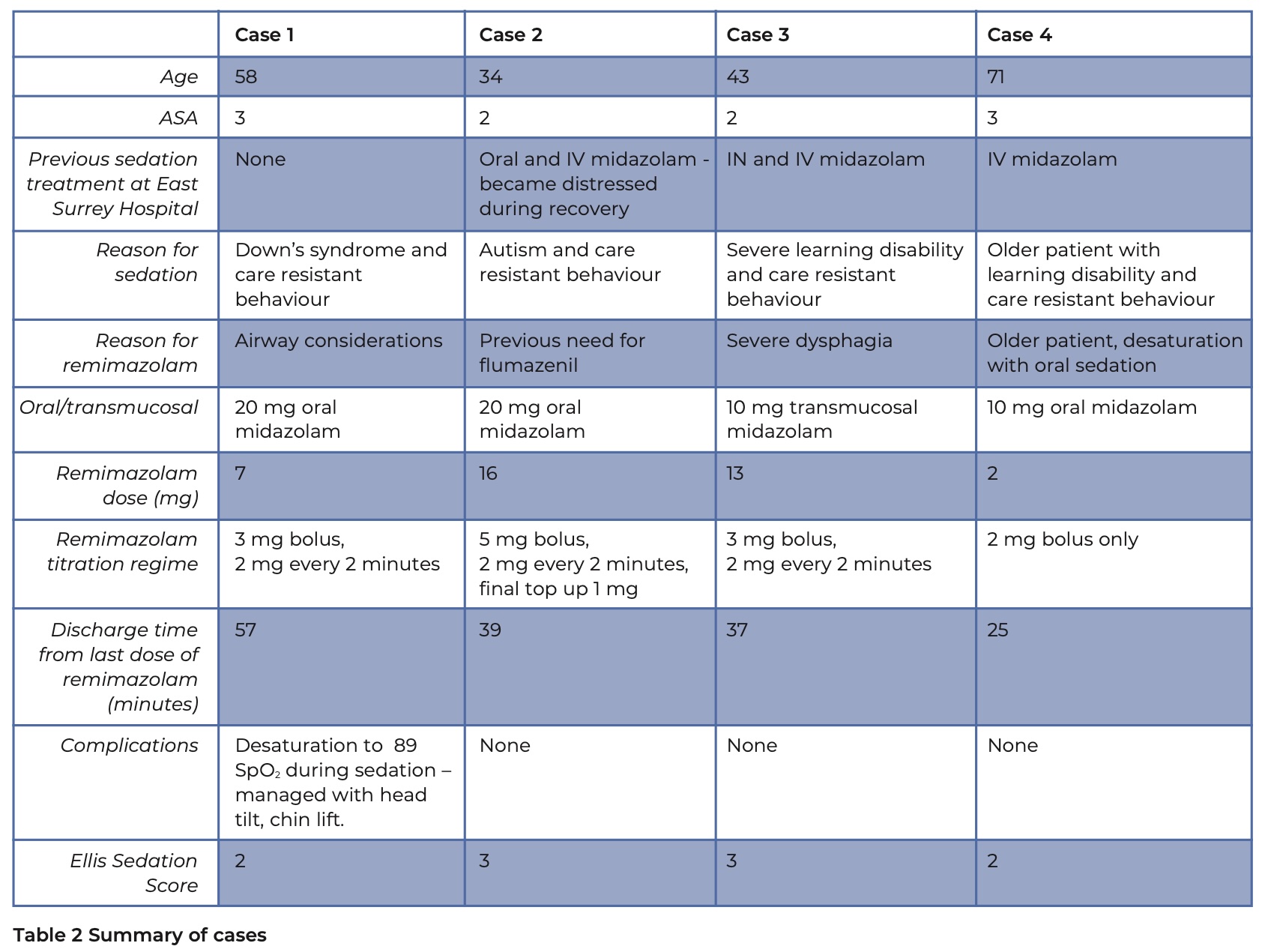
No significant complications were observed, and no supplemental oxygen or flumazenil was required. In case one, there was minimal desaturation, which was managed effectively with a chin lift. Patients with Down’s syndrome are well documented to have short and narrow airways, which can result in difficulties with intubation and an increased risk of respiratory depression or post-operative respiratory tract infections,15 therefore remimazolam was beneficial in minimising the risk of respiratory depression.
Treatment was completed in all cases and included examinations, extractions, scaling, and blood tests. Satisfactory radiographs could not be obtained in cases two and three due to patient movement; however, these patients had also been unable to tolerate radiographs during previous midazolam-only sedation.
Recovery
The recovery time following the last dose of remimazolam ranged from 25 to 57 minutes, with an average of 39.5 minutes. There was no pattern between the total dose of remimazolam or oral / transmucosal midazolam and recovery time. This is higher than reported findings from similar case series, which reported 23 to 27 minutes with remimazolam alone,2, 3 and at the higher end of remimazolam recovery times which are reported to be 10 to 40 minutes. However, this is still shorter than midazolam, which ranges from 20 to 80 minutes.8 The comparatively prolonged recovery is most likely due to the midazolam taking longer to wear off than the remimazolam itself. In all cases, recovery was uneventful and minimised distress for a cohort of patients who all had learning disabilities and were at increased risk of becoming agitated post-operatively.
In patient three, whose treatment lasted under five minutes, remimazolam enabled the completion of care while preventing the prolonged recovery period that might have otherwise occurred. It is often during the recovery phase, when patients are no longer stimulated, that there is a risk of respiratory depression. A shorter, more predictable recovery period is particularly advantageous in older patients. As the special care dentistry population ages, the use of remimazolam may prove increasingly valuable, given that older adults are more sensitive to sedative medications and often experience extended recovery with midazolam.
Limitations
One notable disadvantage of remimazolam compared to intravenous midazolam is its significantly higher cost, with a 20 mg remimazolam vial costing £18.75 versus £1.36 for a 5 mg/5 ml midazolam ampoule at time of writing.16, 17 For context, in our Trust pharmacy the oral formulation of midazolam (Miprosed®) used costs £20.85 per 7.5 ml bottle and a vial of concentrated midazolam 40 mg/ml for transmucosal use costs £26.85 per 0.5 ml vial. In the cases discussed, the decision to use remimazolam was based on improved patient outcomes. For example, in case one, the patient may otherwise have required referral for treatment under anaesthetist-led sedation in a theatre setting, a pathway that would have been far more resource-intensive and costly.
This case series is limited to four patients, and while the initial outcomes are promising, further evaluation is needed. Future research should include larger-scale studies and formal cost– benefit analyses to better understand the value of remimazolam in routine special care dentistry practice.
Conclusion
The combined use of IV remimazolam following oral / transmucosal midazolam in this case series was safe, with no adverse events and successful completion of treatment in all cases. Recovery was uneventful, even among patients with complex needs and a history of prolonged or challenging sedation. However, an important consideration when combining benzodiazepines is that remimazolam’s effects may wear off before the sedative effects of oral or transmucosal midazolam have fully resolved.
Acknowledgements
The authors would like to thank the special care dentistry department at East Surrey Hospital for their support.
Declaration of Interest
The authors declare no conflict of interests.
References
1. Ransford N J, Manley M C G, Lewis D A, et al. Intranasal/intravenous sedation for the dental care of adults with severe disabilities: a multicentre prospective audit. Br Dent J. 2010 Jun;208:565–9. DOI: 10.1038/sj.bdj.2010.501
2. Doshi M, Prasad R, Reilly D. A service evaluation of the use of IV sedation with remimazolam for adults with an acquired brain injury. SAAD Dig. 2025;41. DOI: 10.63507/QLKO2726
3. Liow A M, Akuffo N, Yeo X H, Clough S. Remimazolam as a sedative for dental procedures: a case series. SAAD Dig. 2025;41. DOI: 10.63507/QATP4875
4. Intercollegiate Advisory Committee for Sedation in Dentistry. Remimazolam for intravenous conscious sedation for dental procedures - IACSD standard on clinical use and training [Internet]. 2023. Online information available from: https://www.rcseng.ac.uk/-/media/fds/iacsd/iacsd-remimazolam-statement-130623.pdf (Accessed May 2025)
5. Dao V A, Schippers F, Stöhr T. Efficacy of remimazolam versus midazolam for procedural sedation: post hoc integrated analyses of three phase 3 clinical trials. Endosc Int Open. 2022 Apr;10:E378–85. DOI: 10.1055/a-1743-1936
6. Shehabi Z, Flood C, Matthew L. Midazolam use for dental conscious sedation: how safe are we? Br Dent J. 2018 Jan;224:98–104. DOI: 10.1038/sj.bdj.2017.1042
7. Prommer E. Midazolam: an essential palliative care drug. Palliative Care and Social Practice. 2020 Jan;14:2632352419895527. DOI: 10.1177/2632352419895527
8. Kim K M. Remimazolam: pharmacological characteristics and clinical applications in anesthesiology. Anesth Pain Med. 2022 Jan 31;17:1–11. DOI: 10.17085/apm.21115
9. Zhang L, Li C, Zhao C, You Y, Xu J. The comparison of remimazolam and midazolam for the sedation of gastrointestinal endoscopy: a meta-analysis of randomized controlled studies. Afr H Sci. 2022 Aug 1;22:384–91. DOI: 10.4314/ahs.v22i2.44
10. Timpe Behnen E, Langley J. Ask the Expert: Multiple Benzo Prescriptions. Pract Pain Manag. 2014;14.
11. Long X, Wen L, Yang H, Zhu G, Zhang Q, Jiang J, et al. ED95 of remimazolam in nasal administration for attenuating preoperative anxiety in children. Front Med. 2023 Aug 23;10:1253738. DOI: 10.3389/fmed.2023.1253738
12. Pesic M, Schippers F, Saunders R, Webster L, Donsbach M, Stoehr T. Pharmacokinetics and pharmacodynamics of intranasal remimazolam—a randomized controlled clinical trial. Eur J Clin Pharmacol. 2020 Nov;76:1505–16. DOI: 10.1007/s00228-020-02984-z
13. European Medicines Agency. Byfavo: EPAR - Product Information [Internet]. European Medicines Agency; 2021 [cited 2025 May 31]. Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/byfavo
14. Ellis S. Response to intravenous midazolam sedation in general dental practice. Br Dent J. 1996 Jun 8;180(11):417-20. DOI: 10.1038/sj.bdj.4809108. PMID: 8762804.
15. Pelli M, Loffredo C, Menna C, Fiorelli S, Massullo D. Anesthetic Management of an Adult Patient With Down Syndrome for Thoracic Surgery. Cureus [Internet]. 2021 Aug 12 [cited 2025 Apr 24]; Available from: https://www.cureus.com/articles/46921-anesthetic-management-of-an-adult-patient-with-down-syndrome-for-thoracic-surgery. DOI: 10.7759/cureus.17130
16. Joint Formulary Committee. Remimazolam Medicinal Forms [Internet]. British National Formulary; [cited 2025 May 31]. Available from: https://bnf.nice.org.uk/drugs/remimazolam/medicinal-forms/
17. Joint Formulary Committee. Midazolam Medicinal Forms [Internet]. British National Formulary; [cited 2025 May 31]. Available from: https://bnf.nice.org.uk/drugs/midazolam/medicinal-forms/