
![]()
Please click on the tables and figures to enlarge
The attitudes of doctors and dentists to the use of oral sedatives to control anxiety in minor surgical, imaging and dental surgery
R. Emanuel*1 BDS, MSc, FDS RCSEd.
B. Raveendran2 BDS, PgCert(MedEd), MFDS, DipSCD RCSEd
S. Turkistani3 RDN (Hons), MRes
M. Asbury4 BA(Hons), MA
J. Pateman5 MA MB BChir FRCA
P. Patel6 BDS(Hons), MSc
1Consultant in Special Care Dentistry, Sussex Community NHS Foundation Trust, Brighton General Hospital, Elm Grove, Brighton, East Sussex, BN2 3EW
2Specialty Registrar, Sussex Community NHS Foundation Trust, Brighton General Hospital, Elm Grove, Brighton, East Sussex, BN2 3EW
3Associate Researcher, University of Portsmouth Dental Academy, William Beatty Building, Hampshire Terrace, Portsmouth, Hants, PO1 2QG
4General Manager (Dental Services), Sussex Community NHS Foundation Trust, Brighton General Hospital, Elm Grove, Brighton, East Sussex, BN2 3EW
5Consultant Anaesthetist, University Hospitals Sussex NHS Foundation Trust, Royal Sussex County Hospital, Eastern Road, Brighton East Sussex, BN2 5BE
6Clinical Director, Sussex Community NHS Foundation Trust, Brighton General Hospital, Elm Grove, Brighton, East Sussex, BN2 3EW
*Correspondence to: Dr Robert Emanuel
Email: Robert.emanuel@nhs.net
DOI: 10.63507/MBMK7955
Abstract
Introduction
Dental surgery is a cause of anxiety for many patients as are certain medical procedures. To alleviate anxiety for patients, a small dose of oral sedative can be used. This use, however, will be affected by perceived benefits and barriers to their use.
Aim
The aims of this study were to:
- Explore the attitudes and practices of both dental and medical practitioners regarding using oral sedatives in their day-to-day practice
- Develop a questionnaire based on the qualitative data to be used in planned future quantitative research.
Methods
Qualitative research methodology using semi structured interviews.
Results
A total of 16 practitioners were interviewed (eight doctors and eight dentists). Several themes and sub-themes emerged including similarities and differences between prescribing patterns. The results showed their use was considered advantageous to both groups, but their use was limited to certain circumstances only and routine use was only for very select cases. The barriers to their use were different for both groups but in general they both reported subjective and practical barriers.
Conclusion
Both professional groups occasionally use oral sedatives to aid in anxiolysis.
Key learning points
- Both doctors and dentists value small dose sedatives as useful in anxiolysis for anxious patients. However, their current use is for limited circumstances only
- Both groups report barriers to their use, but these barriers are different for each different professional group
- To improve their future use in dentistry, it was suggested further training and experiential support would be useful.
Introduction
Dental surgery is a cause of anxiety for many patients.1 Although the majority of patients undergo operative dental treatment with local anaesthetic (LA) alone, with no additional anxiety relief, many report levels of anxiety high enough to warrant the use of supplemental techniques to address this.2 The most recent Adult Oral Health Survey3 reported that 42% of adults experienced moderate dental anxiety when faced with dental treatment, whilst a further 12% experienced extreme dental anxiety.
These anxiety-reducing supplemental techniques include:
- Non-pharmacological methods such as cognitive behavioural therapy (CBT)4
- Use of small dose oral sedatives taken prior to the procedure. Arguably the simplest method of pharmaceutical based anxiolysis.5 This is normally classified as ‘pre-medication’ to prevent confusion with true oral sedation as outlined in the IASCD guidelines6
- Use of nitrous oxide inhalation. Especially appropriate for use in children.6 However, potential future difficulties with this technique involve waste gas scavenging and sustainability
- Intravenous (IV) sedation. Effective method of anxiolysis, but additional steps and equipment are necessary6
- General anaesthetic (GA). Considered a last resort method due to limited capacity and high cost and risks, although GA risk is very low for fit patients (ASA 1).7
Dentistry
Issues with providing NHS dental treatment to anxious patients include:
- Limited availability of NHS dentistry for new patients8
- IV sedation is costly and IV services can have very long waiting lists.
The use of a small dose oral sedative as a pre-med has potential to be the least expensive of all the options for anxiolysis, as its available from any pharmacy and will involve no additional procedural time or additional equipment.
Medicine
In medicine the issues around adding an element of sedative use to alleviate anxiety associated with certain procedures include:
- Perceived risk that a sedative pre-med will delay discharge
- Managing patient expectations: treatments previously conducted under general anaesthesia are now often carried out under local anaesthetic (LA).
Although it can be argued that dentistry and medicine are different, many procedures used by both branches of healthcare can cause anxiety, which by its very nature can be an unpleasant experience and possibly could lead to care avoidance behaviour.
Aim(s)
The aims of this study were to:
- Explore the attitudes and practices of both dental and medical practitioners (dentists and doctors) regarding the use of oral sedatives in their day-to-day practice
- Develop a questionnaire based on the qualitative data to be used in planned future quantitative research.
Methodology
A qualitative thematic analysis was carried out based on the semi-structured interviewing of eight (primary care) dental practitioners (dentists - DPs) and eight medical practitioners (doctors - MPs).
Convenience sampling was used from the authors’ professional contacts.
The interviews were recorded and transcribed by members of the group. Transcripts of the interviews as well as the research notes from each session were analysed thematically, using Nvivo 12 to generate themes and subthemes. The use of AI was governed by the recent NICE position statement.9
The interview transcripts were arranged and sorted into NVivo 12 software to run the qualitative analysis. An inductive approach, with the help of line-by-line reading of the interview transcripts, allowed for the development of nodes, segments, codes and classifications. This paper employed Braun and Clarke’s Six-Step Thematic Analysis Framework.10
Results
Most of the participants in this study were experienced professionals, aged between 36 and 62, with an average age of 48. On average, they had 29 years of experience, (range of 10 years to 37 years), with most participants clustered around the higher end of the age range.
Most participants in the study (n = 11) were primarily employed in mixed NHS and private practice settings, while the remaining participants (n = 5) worked exclusively within the NHS. The dentists had the highest frequency of mixed practice, with only one practising in the NHS alone. The doctors were evenly matched with four doing mixed, and four NHS only (Table 1).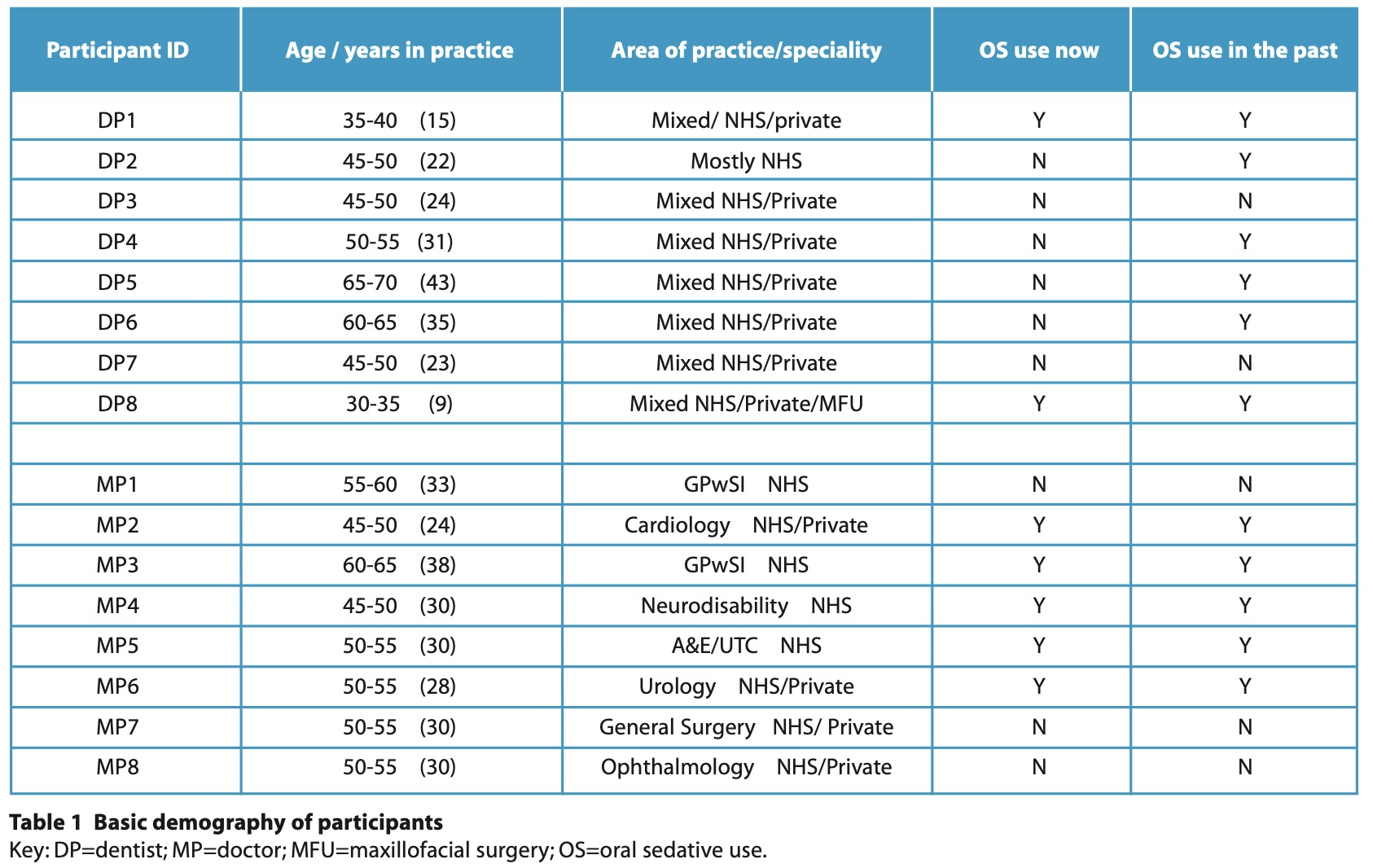
Statistical analysis revealed weak correlations between both age (r = 0.18, p = 0.21) and years in practice (r = 0.22, p = 0.16) with benzodiazepine use. This suggests that practitioner experience does not significantly impact the likelihood of prescribing an oral sedative.
The use of sedatives was assessed across two professional groups: dentists and doctors, with each group consisting of eight participants. Among the dentists, 25% (2 out of 8) reported currently using sedatives, while 25% (2 out of 8) stated that they have never used sedatives. A sizeable portion, 75% (6 out of 8), indicated that they previously used sedatives for procedures such as extractions, and other complex treatments when managing anxious or highly anxious patients. However, four of these dentists no longer use sedatives in their practice. Furthermore, 90% (7 out of 8) of dentists reported that although sedatives were effective in managing anxious patients, they ceased their use due to perceived 'new regulations’.
In contrast, among the doctors, 62.5% (5 out of 8) reported currently using sedatives / sedation in Accident and Emergency (A&E) departments, endoscopy and colonoscopy procedures (IV) but there was often a preference for IV sedation rather than oral pre-medication. Additionally, all those who reported using oral sedatives, stated it was very rare to use oral sedatives rather than routinely, though oral sedatives were more popular to deal with anxiety and claustrophobia associated with MRI scans. 37.5% (3 out of 8) preferred to opt out from using sedatives altogether.
The use of sedatives was widely regarded as beneficial by the participants. Key advantages include improved patient comfort, increased co-operation, cost-effectiveness and a reduction in the need for more invasive forms of sedation. Sedatives were particularly valued for their ability to help anxious patients access care and co-operate during procedures, thus enhancing their overall treatment experience. Notably, 94% (15 out of 16) of participants acknowledged the benefits of sedative use, while only 6% (1 out of 16) disagreed, indicating a strong consensus regarding the positive impact of sedatives in managing patient anxiety and improving treatment outcomes.
Regarding barriers to the use of oral sedatives, 61% (11 out of 18) of participants discussed subjective barriers, while 66% (12 out of 18) discussed practical challenges. Additionally, 44% (7 out of 16) of participants made suggestions to overcome these barriers.
The themes and subthemes identified in this study are systematically summarised and demonstrated in Table 2.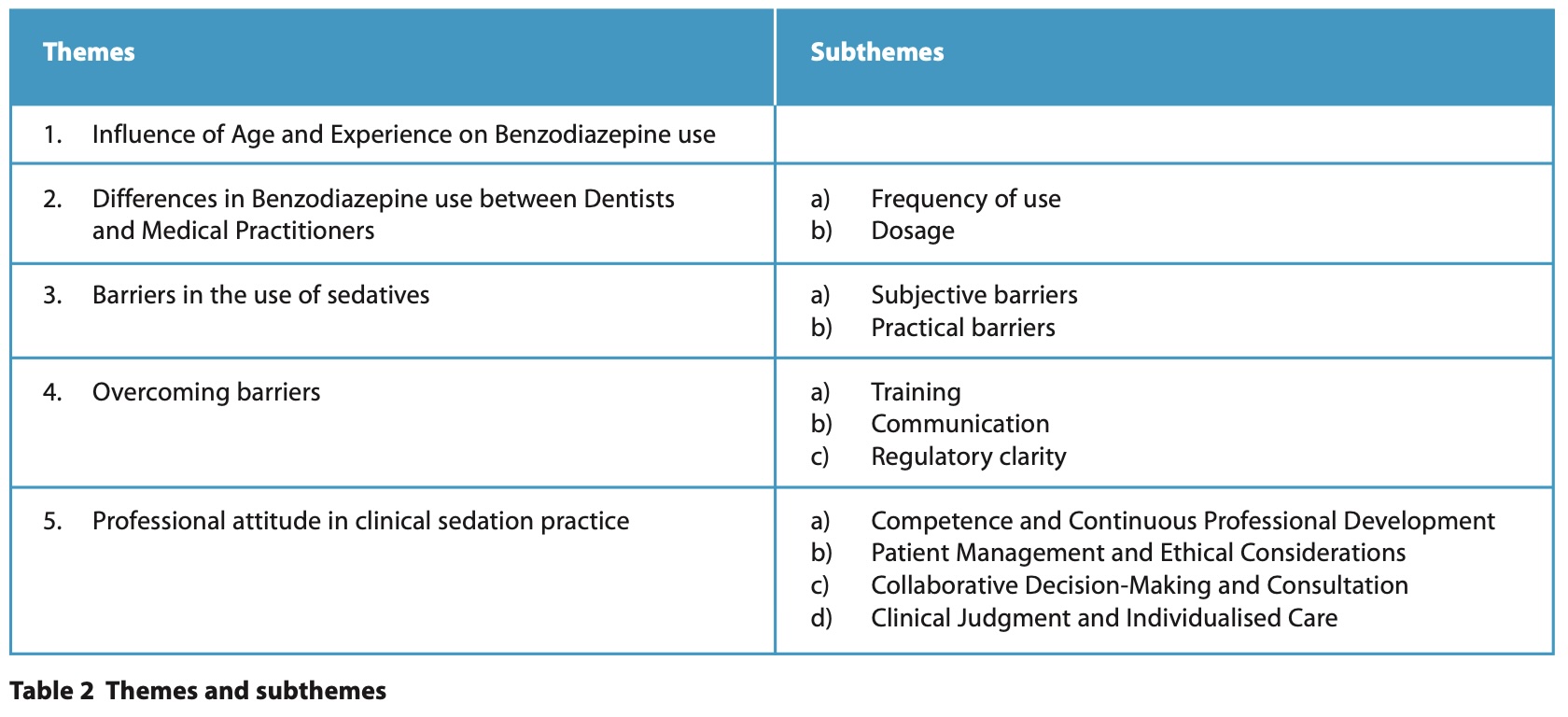
Discussion
Theme 2: differences in benzodiazepine use between dentists and doctors
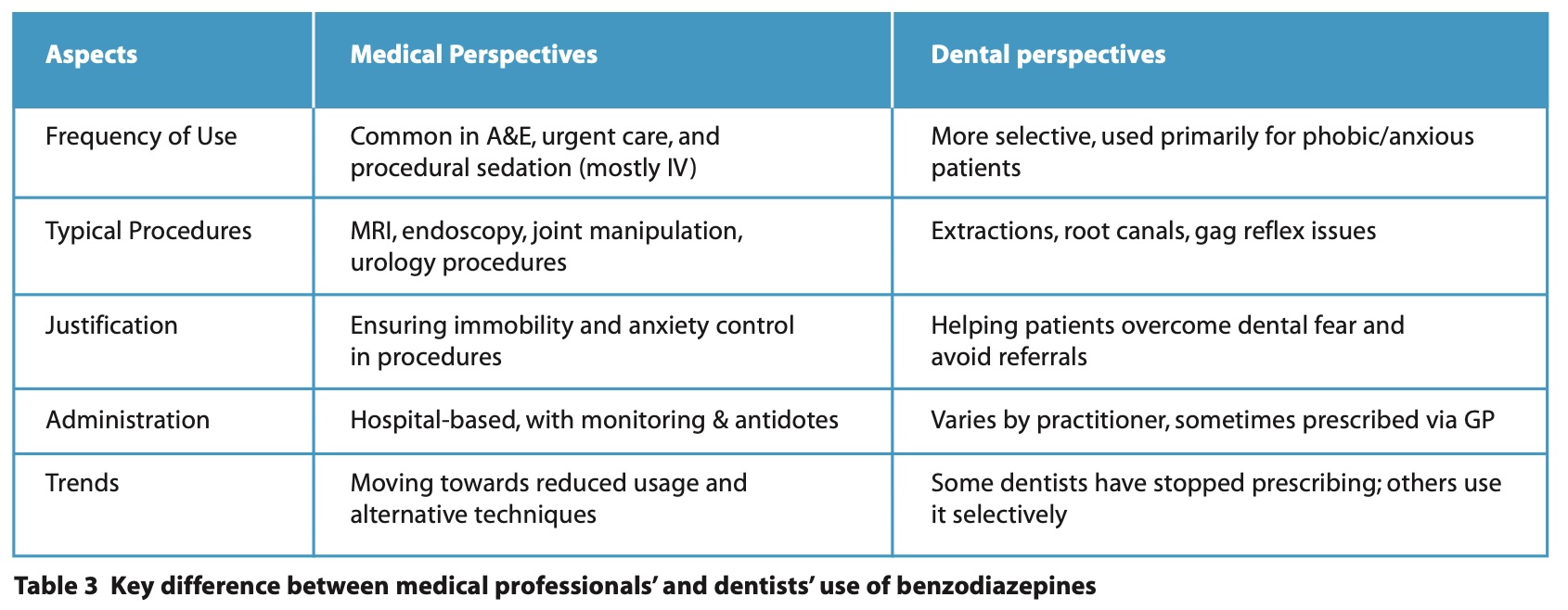
As shown in the results, the data reveals that a higher proportion of doctors currently use sedatives (both oral and IV) more frequently compared to dentists, who often used them in the past. The perspectives of doctors and dentists regarding using benzodiazepines for sedation demonstrated notable differences, reflecting their distinct clinical environments and patient needs (Table 3).
Doctors, particularly those working in urgent care, viewed benzodiazepines as an essential and routinely used tool for managing patient anxiety and facilitating procedures: ‘In urgent care A&E, it is a very common practice, so they see it as a very helpful, useful medication’ MP5.
However, a minority of doctors abstained from oral benzodiazepine use including for procedures such as endoscopy and colonoscopy, where alternative sedation methods, including IV are standard. ‘We only normally use sedatives for endoscopy and colonoscopy, where traditionally we have just followed intravenous sedation, we don’t have many other indications for using oral sedatives’ MP7.
In addition, one participant highlighted a critical concern regarding benzodiazepine use in older patients, emphasising the variability in individual responses even at low doses. ‘Some patients, especially with the older population, even with a low dose of 2 mg can get a little bit confused and might suddenly doze off and wake up with a start in the middle of surgery which can make (for) some scary movements.’ MP8.
In contrast, dentists expressed a more varied perspective, with some recognising the benefits of benzodiazepines in reducing patient anxiety, facilitating co-operation, and improving treatment experiences, particularly for phobic or highly anxious patients.
‘It was just for phobics really, and just people who were really nervous.’ DP4.
Furthermore, some dentists were constrained by prescription requirements, with some indicating that writing prescriptions for benzodiazepines required specificity and were worried about adherence to regulations, including obtaining further qualification.
‘Haven’t done any formal qualification on it.’ DP2. While others believed that the use of sedatives in dental settings is not beneficial. ‘
I don’t think there is huge benefits to be fair.’ DP4.
Overall, while both groups acknowledged the anxiolytic benefits of benzodiazepines, doctors demonstrated greater confidence in their routine use, whereas dentists exhibited a more cautious and selective approach, often shaped by (perceived) regulatory and practical considerations.
Subtheme 2a: the frequency of use
The frequency of the use of sedatives as ‘routine practice’ related terms is cross referenced in Table 4.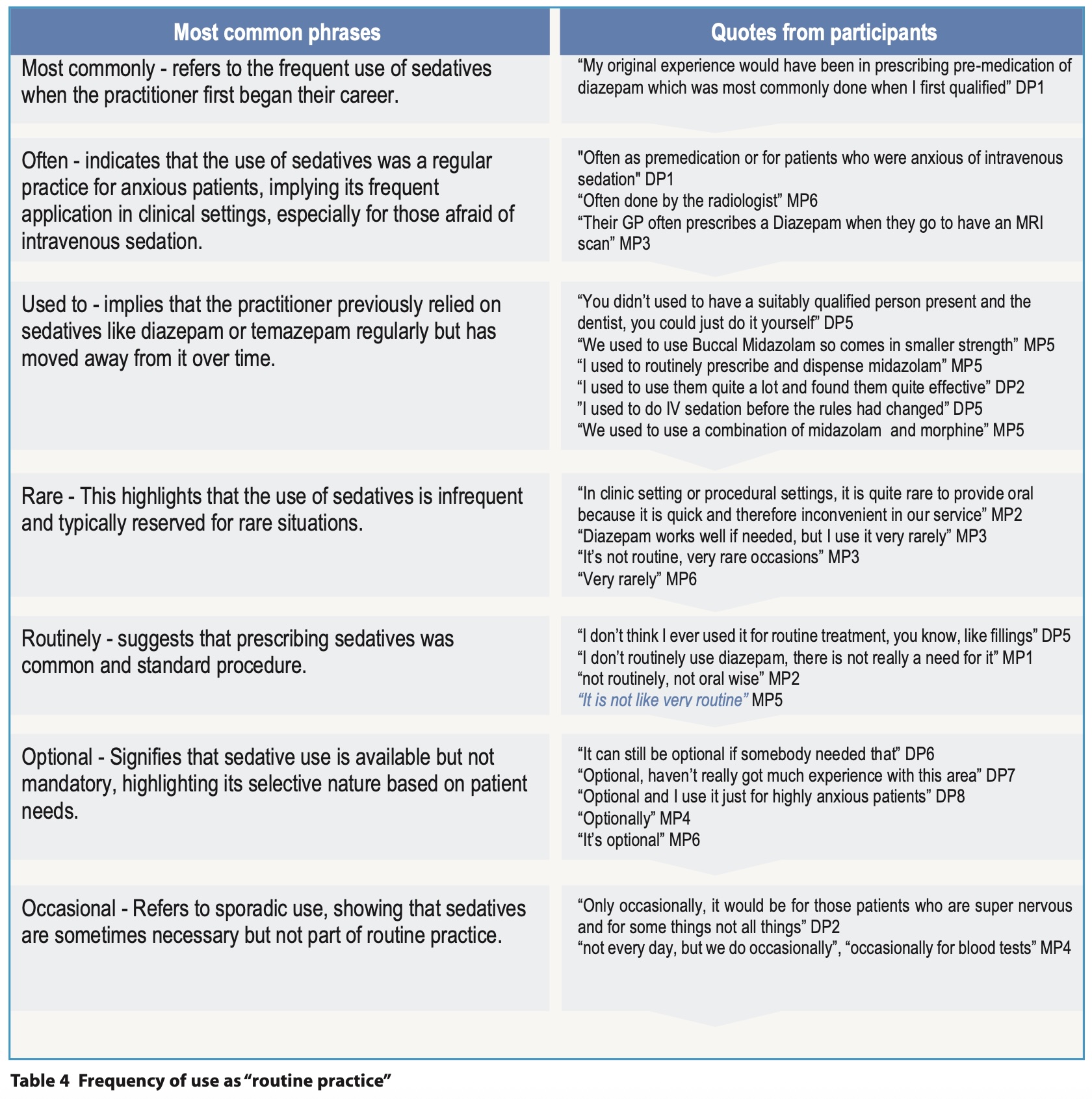
Theme 3: barriers in the use of sedative
The use of sedatives in clinical practice is shaped by various barriers. While benzodiazepines are widely recognised for their effectiveness in alleviating anxiety and facilitating procedures, their use is not without challenges.
Subtheme 3a: subjective barriers
Subjective barriers to sedative prescribing are influenced by clinicians' individual experiences, confidence levels and anxieties surrounding the prescribing process. These barriers often stem from concerns about patient safety, and adherence to regulatory guidelines. They were reported more widely by the dentists rather than doctors.
A significant barrier to the use of sedatives is the lack of adequate training and exposure during undergraduate education, leaving many clinicians uncertain about appropriate prescribing practices.
One participant stated:
‘I don’t think it is something taught very well in undergraduate in my experience having trained dentists for the last ten years from different universities.’ DP1.
“If they are training in an environment that doesn’t do it, they will have no clue potentially how to do it.’ DP1.
Clinicians also express apprehension due to limited awareness of the benefits and concerns over over-sedation. One participant admitted: ‘A lot of my colleagues (are) apprehensive to prescribe it because I think as dentists, we don’t routinely prescribe lots of things.’ DP6.
Another reflected on changes in personal confidence over time: ‘I guess I am a bit more worried now than I was then. I was probably a bit more relaxed about it.’ DP2.
Some practitioners even question the effectiveness of sedatives, believing their effects may be more psychological than pharmacological: ‘In my experience, I just thought it doesn’t work very well. There was just a placebo effect. It’s hard to tell.’ DP4.
This suggests that confidence plays a significant role in the decision to prescribe, and additional training or guidance may be necessary to overcome these subjective barriers.
On the other hand, safety concerns contribute to hesitancy, particularly regarding rare but serious risks of over-sedation. While some acknowledge that benzodiazepines are generally safe, there is fear of potential complications, particularly in inexperienced hands:
‘There is a slight risk if benzodiazepines are safe even with overdose, but people who are inexperienced may fail to recognise that, for example, a patient has had a lot of alcohol that day or other medication which might be causing sedation.’ MP5.
Likewise, arranging for patient supervision post-procedure is another challenge. ‘The other barrier is the patient needs to bring someone with them and to take them back.’ DP6.
Subtheme 3b: practical barriers
In contrast to subjective concerns, practical barriers are logistical and regulatory, impeding the seamless prescription and administration of sedatives in clinical practice. For dentists, private prescriptions are often not accepted by pharmacies, further complicating accessibility for practitioners. ‘The way you would normally write a private prescription is just on letter-headed paper, and in general practice, if you write a controlled drug in a private prescription, the pharmacy won’t take it.’ DP1.
‘Today is physically getting hold of it from pharmacies generally. Prescriptions from dentists not really accepted. Get it from GPs usually, a little bit difficult to get it from us.’ DP3.
‘I got told I couldn’t prescribe that anymore, the pharmacist refused to give me the prescription.’ DP4.
Similarly, practitioners often struggle with prescription protocols and the lack of regular prescribing practice, which can lead to uncertainty regarding appropriate dosing, ‘They don’t know how to write the prescription for it and they don’t know how to utilise it and when it is appropriate to use it.’ DP1.
Beyond prescription and dosing logistics, drug storage requirements pose additional hurdles, especially for those working in a hospital setting. As controlled medications, sedatives must be kept in a secure location, which may not always be feasible. While many participants stated that storage was not a concern since they primarily issued prescriptions, those with the capability to store sedatives encountered distinct challenges.
‘These are controlled medications, so storage needs to be in a locked area, and a register needs to be kept.’ MP5.
‘There was a little bit to do with storage as they were controlled drugs and checking it at the end of the day and so that was an issue.’ MP6.
The increasing demand for sedation exacerbates the issue of poor availability, as more patients become aware of it. ‘The more available it is, the more people will want it.’ DP5.
Finally, practical challenges extend to workforce constraints, where clinicians face increased responsibilities without adequate support. The removal of nursing assistance in some settings, usually amongst doctors, has forced clinicians to scale back their procedural capabilities, impacting sedation use. ‘As you are no longer assisted by a nurse, you will need to reduce what it is you are comfortable to do within a time frame, as by the end of the day, it's about being safe.’ MP1.
These barriers, ranging from insufficient training and institutional constraints to concerns over safety and efficacy, create an environment where many clinicians opt to avoid sedative use altogether.
Theme 4: overcoming barriers
Overcoming barriers to sedation prescription and administration requires a multifaceted approach, integrating structured training, improved accessibility to information and standardised clinical practices. The following strategies, derived from participant insights, provide a framework for addressing these challenges.
Subtheme 4a: structured training and mentorship
A lack of clinician confidence due to insufficient training was identified as a key barrier to effective sedation use. One participant emphasised the value of clear instructions and professional support. ‘I've had more advanced training prescribing so to me it's an easy prescription to write but I suppose if I hadn't had that training maybe I would need some training.’ DP8.
‘I don’t think there should be any barrier but the person doing it should need training and knowledge of the medication.’ MP5.
Providing ongoing training opportunities can facilitate experiential learning, ensuring that clinicians gain the necessary competence and confidence to administer sedation safely. ‘The junior doctor would do the prescribing and be present, and then all the staff would go onto a sedation course, which they had to do annual renewal of that training.’ MP6.
Subtheme 4b: communication
Effective communication plays a crucial role in overcoming barriers related to sedation use. This includes both patient education and the dissemination of information among healthcare providers. Providing patients with clear, comprehensive information about sedation options can empower them to make informed decisions.
Encouraging pre-procedure testing of sedatives was proposed to enhance safety and predictability. ‘Ask patients to try it on a day other than procedure day to see how they respond, because if they haven’t had it before, you don’t know how they will respond.’ MP3.
By improving communication and education at all levels, both patient confidence and clinician preparedness can be enhanced, leading to better procedural outcomes.
Theme 5: professional attitude in clinical sedation practice
Professional behaviour in clinical sedation practice is characterised by a combination of expertise, patient-centred care, adherence to regulations and collaborative decision-making. Participants highlighted several key aspects that demonstrate professionalism in managing sedation practices in dental and medical settings.
Subtheme 5a: competence and continuous professional development
A foundational aspect of professional behaviour is maintaining clinical competence through formal education and ongoing training. One practitioner emphasised the value of professional qualifications, stating how structured training contributes to practitioners’ confidence and ability to provide safe sedation. ‘I’ve done the sedation diploma, and I’ve got SAAD training, so I feel very comfortable with it.’ DP8.
Mentorship also plays a crucial role in skill development. A clinician reflected on their early career, suggesting that guidance from experienced colleagues strengthens clinical decision-making and ensures best practices. ‘Maybe have clear instructions on how to do that, and maybe have someone mentor you, it will be helpful too.’ DP1.
Additionally, continuous education allows practitioners to make informed decisions regarding sedation protocols, dosage adjustments, and patient safety.
Subtheme 5b: patient management and ethical considerations
Professionalism in sedation includes careful patient selection and ethical considerations regarding the use of sedatives, demonstrating a commitment to patient-centred approach using sedation only when necessary, rather than as a default option. ‘Many of my patients cope with just a bit more calm, a bit more time, and I put in a little bit longer and do things slowly, rather than the ones that are so extreme, probably where I need to refer onwards for treatment.’ DP7.
Additionally, clinicians recognise the importance of trialling sedative effects before a procedure. Practitioners took precautions that reflected a professional duty to minimise risk and enhance patient safety. ‘Several days before the procedure, take one and ask your friends, family, husband, or wife to observe how you react.’ MP3.
Subtheme 5c: collaborative decision-making and consultation
Professionals feel strongly for the need for institutional protocols to support sedation in medical procedures. One clinician suggested that structured approaches to sedation improve patient compliance and experience over time. ‘If we do it as part of the standard processes, it helps a lot of people accept the investigation, particularly if it is for something that is going to be a repeat attendance.’ MP6.
Therefore, professional behaviour in sedation practice is demonstrated through competence, adherence to ethical and regulatory standards, collaborative decision-making and a commitment to individualised patient care.
Subtheme 5d: clinical judgment and individualised care
Professional behaviour in sedation practice also involves individualised patient care and recognising that sedation should be tailored to specific needs. The impact of sedation on long-term patient experiences was acknowledged, reflecting an awareness of how sedation decisions affect patient perceptions and future medical compliance.
‘If an MRI scan will need to be repeated for two- or three-year interval to see if there is a change, you want that to be a positive experience, so sometimes the impact it might have on recall for the patient to not have a bad experience, it would be beneficial.’ MP6.
Conclusion
This study aimed to explore dentists’ and doctors’ attitudes to using small dose oral sedatives. The themes which developed highlighted both similarities and differences between both professional groups.
Similarities included recognition of the potential use of small dose benzodiazepines as a pre-med for anxiolysis, but also their relatively infrequent use and only for certain procedures.
Differences included not only the subjective and practical barriers of use but the solutions for overcoming these barriers.
Limitations
There is perhaps a risk of bias caused by convenience sampling. This led to the dentists being recruited via the Local Dental Committees of East and West Sussex and therefore may represent a similar group of very engaged professionals. The doctors were also selected via convenience sampling, but were arguably a more diverse mix of hospital consultants, Trust consultants working in urgent care and rehabilitation as well as GPs with special contracts for minor surgery.
Follow up
This project will inform development of a questionnaire to be used nationally to explore current practice within dentistry, identify areas for teaching and learning and provide evidence to improve access for all dental patients to inexpensive and timely anxiety management. This hopefully should enable dentists to gain expertise and, perhaps more importantly, confidence in using small dose, pre-med oral sedatives in their practice.
Ethics declaration
Health Research Authority and Health Care Research Wales Approval issued: IRAS 339061.
Declaration of Interests
The authors declare no personal conflict of interests.
The research was funded by a research grant from The Society for Advancement of Anaesthesia in Dentistry (SAAD).
Acknowledgements
We would like to thank Helen Vaughan, Research & Development manager at Sussex Community NHS Foundation Trust, for her assistance at many crucial points during the process of preparing and carrying out the research.
References
1. White A, Giblin L, Boyd L. The prevalence of dental anxiety in dental practice settings. J Dent Hyg 2017; 91: 30-34.
2. Fiorillo L. Conscious sedation in dentistry. Medicina 2019;55(12):778. doi:10.3390/medicina55120778.
3. Office for Health Improvement and Disparities. Adult oral health survey 2021: service use and barriers to accessing care. London: UK Government; 2021. Available from: https://www.gov.uk/government/statistics/adult-oral-health-survey-2021 (accessed March 2025).
4. Hare J, Bruj-Milasan G, Newton T. An overview of dental anxiety and the non-pharmacological management of dental anxiety. In: Renton T (ed). Optimal pain management for the dental team. Cham: Springer; 2022. pp 69-77. doi:10.1007/978-3-030-86634-1_6.
5. Emanuel R. Simplifying anxiolysis for everyday dental practice: a personal and professional perspective. BDJ In Pract 2022; 35: 10-11. doi:10.1038/s41404-022-1786-8.
6. Intercollegiate Advisory Committee for Sedation in Dentistry. Standards for conscious sedation in the provision of dental care. Version 1.1. The dental faculties of the royal colleges of surgeons and the Royal College of Anaesthetists; 2020. Available from: https://www.saad.org.uk/IACSD%202020.pdf (accessed March 2025).
7. Geddis-Regan A, Gray D, Buckingham S, Misra U, Boyle C, British Society for Disability and Oral Health. The use of general anaesthesia in special care dentistry: clinical guidelines from the British Society for Disability and Oral Health. Spec Care Dent 2022; 42(Suppl 1): 3-32. doi:10.1111/scd.12652.
8. Howard S. The dentistry crisis “lapping at the doors of primary care.” BMJ 2022; 377: o1249. doi:10.1136/bmj.o1249.
9. National Institute for Health and Care Excellence (NICE). Use of AI in evidence generation: NICE position statement. Version 1. 2024 Aug. Available from: https://www.nice.org.uk/about/what-we-do/our-research-work/use-of-ai-in-evidence-generation--nice-position-statement (accessed March 2025).
10. Naeem M, Ozuem W, Howell KE, Ranfagni S. A step-by-step process of thematic analysis to develop a conceptual model in qualitative research. Int J Qual Methods 2023; 22: 1-18. doi:10.1177/16094069231205789.