DOI: 10.63507/XIAI3917
A synopsis of articles of interest from the last twelve months
to inspire further reading

Conscious sedation teaching in dental schools of the United Kingdom and Ireland: an update
Taylor K, Dargue A, Vincent A.
Br Dent J 2025; 239: 61-65.
DOI: 10.1038/s41415-025-8400-5
Abstract
Aim
To examine the current state of conscious sedation teaching to undergraduates in the dental schools of the United Kingdom (UK) and Ireland.
Background
In 2000, Leitch and Girdler published ‘A survey of the teaching of conscious sedation in the United Kingdom and Ireland’ in the British Dental Journal, which gave insight into the undergraduate experience and the teaching of conscious sedation in UK and Ireland at that time. In October 2022, the Dental Sedation Teachers Group (DSTG) adapted this survey for the wider dental team to evaluate current undergraduate conscious sedation education in dental schools in the UK and Ireland.
Methods
A survey was adapted and piloted by two DSTG school representatives. This was distributed via email to the DSTG school representatives of UK and Irish dental schools, with repeat emails sent to non-responders.
Results
In total, 13 out of 16 schools responded. Most sedation teaching was led by staff from oral surgery and paediatric dentistry (nine schools). This survey included the wider dental team; sedation training was delivered by staff from hygiene and therapy departments in three schools.
Conclusion
Decreased sedation experience was observed in most schools over the last 25 years. Currently, there is limited experience of undergraduate sedation in most schools.
Reviewer’s evaluation, opinion and points of interest
Dental graduates are not required to provide conscious sedation but must be able to assess anxiety, discuss sedation options and refer patients appropriately. They also need basic knowledge and exposure to sedation for managing anxious or unco-operative patients.
Hygienists and therapists require further training in inhalation sedation but share responsibilities in assessing anxiety and communicating sedation risks.
The findings of this study are concerning because, over the past 25 years, undergraduates have had fewer opportunities for hands-on experience with conscious sedation, largely due to increased pressures on dental schools. In other words, many graduates either lack appreciation of how effective sedation can be for treating anxious patients or, if they do appreciate its importance, don't feel inclined to pursue further training in sedation on their own. Studies indicate that more undergraduate experience with sedation increases confidence and satisfaction, highlighting the need for better training opportunities and postgraduate encouragement.
The survey revealed notable differences in dental students' exposure to intravenous and inhalation sedation. Only one school provided substantial hands-on training in intravenous sedation, and several were unclear about student participation. Both types of sedation experience have declined compared to previous surveys. Only four schools now have dedicated sedation departments. Most staff consider current training adequate, though many would expand it if given more resources.
The authors point out that there is an educational dilemma in that UK dental schools follow flexible GDC guidelines, leading to varied interpretations, especially for practical experience regarding sedation training. Contributing challenges include large class sizes, understaffing, patient non-attendance and other issues. Students’ clinical exposure varies widely.
The necessity for sedation in dental care for anxious patients is clear; however, NHS primary dental services face significant challenges as a result of scarce resources and restricted conscious sedation options. Inhalation sedation remains an important modality for paediatric patients, yet few hospital trusts provide this service, leading to increased reliance on general anaesthesia and rising costs. There is a compelling case for expanding and enhancing sedation services within primary care. An increase in the number of graduates who have received thorough training in sedation during dental school would significantly contribute toward achieving this goal.
FA
Avoiding repeat general anaesthetics in children: a service evaluation of repeat general anaesthetics for dental care in paediatric patients between 2017–2023 in Cardiff Avoiding repeat general anaesthetics in children: a service evaluation of repeat general anaesthetics for dental care in paediatric patients between 2017–2023 in Cardiff
Teague H, Ezzeldin M, Collard M
Br Dent J 2025. Online ahead of print.
DOI: 10.1038/s41415-025-8407-y
Abstract
Introduction
Children may require general anaesthetic (GA) for dental care for a variety of reasons, including limited cooperation or dental anxiety. However, GA is not without risk and to avoid repeat GAs, we must treatment plan effectively. Repeat GAs not only present risks to the child’s health and wellbeing but have economic implications and affect service provision.
Aims and objectives
To determine the incidence of repeat GAs for dental care in paediatric patients, identify why repeat GAs were required and ascertain whether changes need to be made to the treatment planning process.
Methods
Theatre software was used to identify paediatric patients who were booked more than once for dental treatment under GA between 2017-2023. The files of these patients were investigated to ascertain the circumstances leading to the repeat GA procedure.
Results
In total, 41 children (1.21%) had repeat GAs within the six years investigated. Additionally, 51% (n = 21) of paediatric patients requiring a repeat GA had behavioural factors and the most common reason for repeat GAs was new carious lesions.
Conclusion
We have a low repeat GA rate and have been able to identify the most common reasons for repeat GAs, as well as the specific groups of patients commonly requiring them. We have used this information to change our prevention strategies and now discuss cases of repeat GAs among consultant colleagues.
Reviewer’s evaluation, opinion and points of interest
Over six years, 3,402 children received general anaesthesia (GA) for dental care in Cardiff; 41 (1.21%) had repeat GAs, mainly due to new carious lesions (56.1%). Of those with repeat GAs, 51% had behavioural factors such as ASD. The two-year repeat GA rate was 0.26% (n = 9). After excluding cases with complex needs or unpreventable conditions, 16 children (0.47%) had ‘preventable’ repeat GAs.
The paper mentions that although there is no established standard for repeat general anaesthetics (GAs) in paediatric dental care, it is considered best to avoid a second GA in children under five and within two years of the first. The authors advocate appropriate treatment planning to reduce the risk of repeat general anaesthetics. The British Society of Paediatric Dentistry advises comprehensive dental assessments before GA to address all dental disease and minimize repeat procedures. The Royal College of Anaesthetists notes that unnecessary GAs should be avoided due to associated risks, especially for lengthy procedures or younger children. Repeat GAs also increase healthcare costs, with average NHS expenses for multiple extractions in under-18s exceeding £2,000 in 2021.
In an attempt to address this situation in the Cardiff unit, a standardised new patient proforma was introduced over six years aimed at improving departmental record-keeping.
However, documentation of social history, especially for children living in multiple households or with social worker involvement, remains challenging as it has limitations with regard to consent, safeguarding and conveying effective preventive advice.
Paediatric specialists or consultants now oversee GA treatment planning in Cardiff, possibly explaining the lower repeat GA rate compared to units without this approach. A new oral health prevention leaflet is now provided to families at each GA. Repeat GAs are reviewed monthly by all clinicians to discuss treatment planning and support ongoing service improvements.
Prior studies also link specialist-led planning to reduced repeat procedures. The evaluation also shows that repeat GAs are mainly due to failed oral health prevention and it is concerning that repeat general anaesthetics are most often required due to new carious lesions, accounting for 56.1% (n = 23) of repeat cases.
An argument presented in the paper is that ‘repeat GAs often mean children are experiencing dental pain while waiting for treatment and that this may contribute to reduced educational attainment and time out of employment for parents’. However, the question is why should there be waiting time for children who are in dental distress, is that not an inadequacy of the GA service? It was not in the scope of the study to discuss alternative methods of treatment including paediatric sedation. While accepting that some children may be co-operative for treatment under local anaesthetic, other children may never become co-operative due to behavioural needs and for whom GA might be necessary. However, besides focusing on prevention and sound treatment planning, it is essential that every effort is made to improve and enhance paediatric sedation services in community and primary care.
FA
General anaesthesia in special care dentistry. Part 2: delivering dental care
Shehabi Z, Doshi M, Liu S, Geddis-Regan A.
Dent Update 2025; 52: 35-40.
DOI: 10.12968/denu.2025.52.1.3
Abstract
The use of general anaesthesia (GA) in dental care needs to be cautiously justified and considered. Preparation for GA can take a considerable degree of planning, especially as the increased prevalence of co-existing systemic diseases in people with disabilities can increase the risks and challenges of care delivery. When a GA has been deemed appropriate and consent has been gained for relevant treatment, providing treatment this way requires further considerations related to anaesthesia and dental care. There is also a recovery period after GA, and there can be additional post-operative considerations. This paper details the ‘how’ of delivering care under GA, including the dental team's role in supporting an anaesthetic team, the delivery of dental procedures, and the logistics of post-GA care.
Reviewer’s evaluation, opinion and points of interest
This is one of three articles in a series which cover the justification for general anaesthesia in special care patient groups, its administration, and provides a case series to highlight some of the challenges encountered by clinical teams, whilst drawing upon current national guidance and policies in the United Kingdom. Collectively, this is a very useful learning resource, which is enriched by high quality photographs to further aid reader understanding.
I think this is particularly helpful for teams encountering patients with disabilities across all dental specialties, as it can help inform some of the initial discussions with patients or their family / carers and indeed between the dental and anaesthetic teams. In particular, I recommend this series to any readers who are preparing for related professional examinations, as it provides succinct information in a format that is easy to read and retain.
SC
The successful anesthetic management of an adult with Cri-du-Chat syndrome by using personalized behavioral strategies: a case report
Mavridou P, Exarchos C, Kitsakou P et al.
Cureus 2025; 17: e91969.
DOI:10.7759/cureus.91969
Abstract
Cri-du-Chat syndrome (CDCS) is a rare genetic disorder caused by a partial deletion of the short arm of chromosome 5, and it is characterized by craniofacial dysmorphism, severe intellectual disability, and behavioral challenges. Anesthetic management in adults with CDCS is rarely reported, as the literature mostly focuses on pediatric cases. We describe the case of a 34-year-old male with CDCS who was scheduled for periodontal surgery under general anesthesia; he refused all pharmacological premedication and exhibited severe separation anxiety. A caregiver-guided behavioral approach using repetitive familiar phrases enabled a calm transfer to the operating room and successful intravenous access. Anticipating a difficult airway due to micrognathia, macroglossia, and a high Mallampati score (III), nasotracheal intubation was achieved uneventfully. Anesthesia was maintained with sevoflurane and opioid-free analgesia. Recovery was smooth, and same-day discharge was accomplished. This report emphasizes the importance of non- pharmacological preparation, meticulous airway planning, and fast-track anesthetic strategies in adult CDCS patients who cannot tolerate conventional premedication.
Reviewer’s evaluation, opinion and points of interest
Most published cases which describe the features and challenges brought by rare syndromes are limited to paediatrics. The rarity of syndromes is also reflected in the limited clinical exposure, especially concerning anaesthetic management in adult patients, making risk assessment and treatment delivery complex.
Although this article offers relevant detail about the patient’s airway and anaesthetic management with details specific to Cri-du-Chat syndrome, I found it particularly helpful to understand the pre-operative planning with care givers.
The clinical team had a detailed meeting about how to support the patient on the day of admission. They understood the patient’s level of understanding, communication ability and anxiety triggers, such as unfamiliar environments, resistance to touch by strangers and previous episodes of aggression when separated from family. They also learned that the transfer to the operating room posed the greatest challenge, as the patient refused oral or intramuscular sedatives and inhalational induction was impractical due to the patient’s tendency to push masks away forcefully and the patient also exhibited severe separation anxiety. They noted that specific stereotyped phrases and a simple rhythmic children’s song consistently calmed the patient. The anaesthetic team incorporated these cues into the peri- operative plan. On the day of surgery, the anaesthetist and theatre nurse repeatedly used these familiar phrases while holding the patient’s hands, allowing them to walk into the operating room, accompanied by a family member. Continuous repetition of the song and phrases facilitated smooth cooperation while the patient remained seated for the application of monitors and successful intravenous cannulation, enabling immediate administration of induction agents.
This is a great case to remind us all that we cannot rely on pharmacology alone. It is helpful to have access to relevant case reports such as this, to inform planning for future adult patients with rare syndromes.
SC
Anesthetic management of extreme obesity: a case study
Alessandro N M M D, Landsbergen E, Dhumak V.
Int J Anesth Clin Med 2025; 13: 46-57.
DOI: 10.11648/j.ijacm.20251301.17
Abstract
Obesity and Autism Spectrum Disorder (ASD) are prevalent conditions that significantly impact anesthetic management due to airway challenges, metabolic risks, and behavioral considerations. Obesity affects 42% of U.S. adults, while ASD prevalence in adults is approximately 2.21%, necessitating tailored perioperative care strategies. We describe the anesthetic management of a 30-year-old male with a BMI of 101.1, weighing 707 lb (320.7 kg), measuring 5' 9" (1.75 m) and ASD undergoing dental surgery. Preoperative challenges included obesity-related airway risks and communication barriers due to ASD. Despite preoperative preparation, the patient was uncooperative, requiring anesthesia induction on a transport cart. General anesthesia was administered using a rapid-sequence intubation technique with succinylcholine, and airway management was facilitated with ramp positioning. Intraoperative care included sevoflurane, along with adjunctive infusions of propofol, dexmedetomidine, and boluses of fentanyl. Postoperative recovery was uneventful, with stable vitals and effective pain management. Patients with both obesity and ASD present unique anesthetic challenges, including increased airway management risks and behavioral sensitivities. Effective strategies include individualized preoperative preparation, the use of anxiolytics like midazolam, and vigilant intraoperative monitoring. Postoperative care requires careful pain assessment, as individuals with ASD may express discomfort atypically. This case highlights the importance of interdisciplinary collaboration and adherence to obesity-specific perioperative guidelines to optimize outcomes. Further research is needed to establish tailored guidelines for managing individuals with extreme obesity and ASD undergoing surgical procedures.
Reviewer’s evaluation, opinion and points of interest
This publication particularly caught my eye, as many of the issues described have become an increasingly frequent part of my work within special care dentistry. The combination of obesity and autism spectrum disorder (ASD) profoundly impact anaesthetic decision-making, requiring individualised approaches to optimise patient safety and clinical outcomes.
The authors provide some useful background for the increased risk of obesity in adults with ASD including limited physical activity, restricted eating habits, and a preference for high- calorie, low-nutrient foods. Here the authors also highlight how people with ASD often take medications, such as risperidone and aripiprazole, to pharmacologically manage behaviours which can cause metabolic shifts and lead to increased body mass. There is occasionally a complex relationship between how food is handled in the residence in context of behaviour management and may lean towards safeguarding concerns in some situations, where the individual lacks capacity to understand the implications of food-related behaviours.
A structured overview of the anatomical and physiological changes associated with obesity is provided, leading to difficult airway management as well as how to carry out effective pre- operative assessment for morbidly obese patients, strategies for airway management for intubation and other problems that can arise in this group during the peri-operative period such as altered pharmacokinetics, opioid sensitivity and potential delayed emergence from anaesthesia. This is supplemented with a detailed case study of a 30-year-old patient, weighing 323 kg, which is very insightful.
Overall, I found this publication to be a useful summary of the challenges in this patient cohort. Beyond obesity alone, we know that adults with ASD face other significant health challenges and risks associate with anaesthesia. Perhaps weight loss drugs may become more common within this group as part of their pre-operative care plans in order to help reduce some of these risks?
SC
Interdisciplinary management of patients with special healthcare needs undergoing dental treatment in a tertiary care hospital setting in Germany: a retrospective study
Schulz‐Weidner N, Hofmann M, Uebereck C, Krämer N, Schlenz, M A, Becker V, Edinger F, Leicht D, Müller M F, Zajonz T S.
Eur Arch Paediatr Dent 2025; 26: 547-557
DOI: 10.1007/s40368-025-01023-8
Abstract
Purpose
The aim of this retrospective study was to analyse the dental and medical parameters, including peri- and post-operative management and complications, of patients with special healthcare needs receiving dental treatment in a tertiary care hospital setting.
Methods
A total of 154 patients (mean age 7.8±4.1 years) who received dental treatment under general anaesthesia or analgosedation at the Department of Paediatric Dentistry of the XXX University in XXXXXXX between 2021 and 2023 were divided into the following diseases: metabolic disease, nervous system disorder, congenital heart disease, tumour disease, gastroenterological disease, genetic syndrome, pulmonology disease and coagulopathy. Caries experience (dmf-t/DMF-T), type of anaesthesia and pre- and peri-operative parameters were recorded.
Results
Regardless of disease, all children showed higher caries experience in the primary dentition compared to permanent dentition (mean ± standard deviation; 6.44 ± 4.85/2.01 ± 3.87). Most of the children suffered from genetic syndrome, followed by congenital heart and metabolic disease. Dental treatment was mostly performed under general anaesthesia. 92.2% of those patients were intubated orotracheally and 66.9% received antiemetics. The complication rate was lower than 3%.
Conclusions
Data show that special health care needs patients regardless of kind of disease are highly affected by caries and require dental treatment. Most dental restorations were performed under general anaesthesia. Regardless of disease and type of anaesthesia, the complication rate was low, which underlines the high clinical relevance of adequate dental care under general anaesthesia for this vulnerable patient group.
Reviewer’s evaluation, opinion and points of interest
This study reported the care of 154 patients treated over a three-year period based on a retrospective analysis of records.
The review showed that the patients with pre-existing co- factors had a significantly greater level of dental caries than the healthy population. In this review almost 93% were treated under general anaesthesia with the majority (61%) undergoing both restorative and surgical treatments. Sedation was used for a minority of patients with less extensive disease. The age range of the patients was 1-23 years with a mean of 7.4 years. It would have been interesting to see a better breakdown of patient age.
The DMFT or dmft of the patients was almost exclusively the D or d component indicating a need for preventive and earlier access to dental care.
The complication rate was 3%, but the sample is too small to draw conclusions regarding safety of GA in dentistry.
The study does add evidence for the need for dental services for children with medical comorbidities as well as early preventative interventions.
NDR
Effect of pre-cooling the anesthetic agent in comparison to increasing the dosage on the success rate of inferior alveolar nerve block using articaine in mandibular first molars with symptomatic irreversible pulpitis: a double-blind, randomized, controlled clinical trial
Fattahi B, Ghasemi N, Shakouei S, Moghaddam M L
J Endod 2025; 51:989-995
DOI: 10.1016/j.joen.2025.05.011
Abstract
Introduction
Achieving anesthesia in mandibular molar teeth with irreversible pulpitis has been challenging. This study aimed to compare the efficacy of precooling articaine and increasing its dosage for inferior alveolar nerve block (IANB) in the mandibular first molars with symptomatic irreversible pulpitis.
Methods
In this randomized double-blind clinical trial, 90 first mandibular molar teeth with symptomatic irreversible pulpitis (visual analog scale >54) were randomly divided into three groups and received conventional IANB injection with 1.8 mL (1 cartridge) 1C group or 3.6 mL (two cartridges) 2C group of 4% articaine with 1:200,000 epinephrine with room temperature or 1.8 ml of the same agent with 4°C temperature cold cartridge (CC) group. The patients recorded their pain during the injection and access cavity preparation, pulp chamber, and root canal entrance using a visual analog scale. Data were analyzed by repeated measure of analysis of variance and Bonferroni tests (P < .05).
Results
In all three groups, the pain levels at different injection times were significantly different (P < .05). The pain level did not differ significantly between the 2C group and the CC group (P > .05), but the difference was significant between the 1C group and 2C groups (P < .05) and also between the 1C group and CC group (P < .05).
Conclusions
Administration of cold articaine provides a significantly higher success rate of IANBs in mandibular first molar teeth with symptomatic irreversible pulpitis compared to IANB with articaine kept at room temperature; however, increasing the dosage of articaine led to a significantly higher success rate.
Reviewer’s evaluation, opinion and points of interest
The temperature at which local anaesthetics are injected has long been an issue that has been discussed. There have been anecdotal reports that warming local anaesthetics has reduced discomfort during injection, as well as counter claims that, provided the temperature extreme has not been too wide, patients do not notice any difference.
The patients in this study who received the cold local anaesthetic solution reported less pain during injection than the other two groups.
Whilst the cold local anaesthetic group experienced significantly less pain than the single cartridge group, the most effective of the three treatments was two cartridges of local.
The danger of repeated injections is that they are associated with a greater degree of non-surgical paraesthesia post treatment, thus if they can be avoided there is an advantage.
NDR
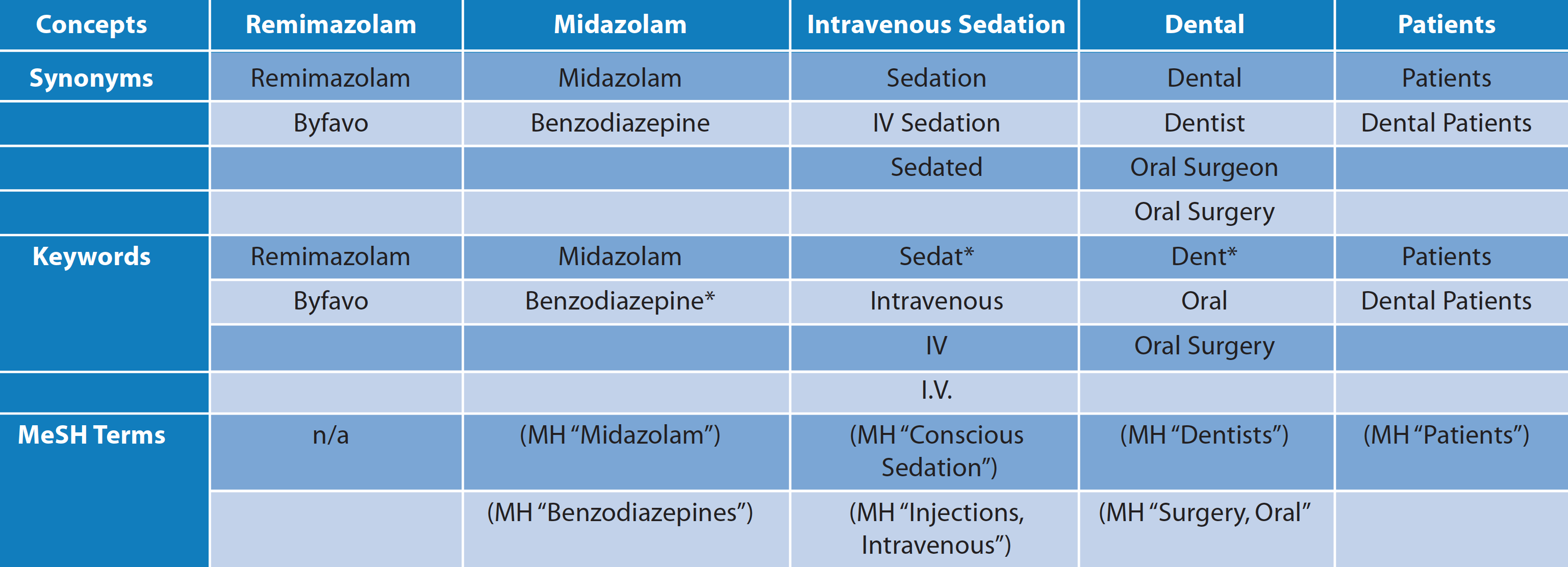
Evaluation of the safety and efficacy of remimazolam combined with remifentanil for sedation in adult dental anxiety patients undergoing mandibular impacted third molar extraction: a single-center, retrospective cohort analysis
Chen C, Chu-Xiong P, Wen-Jing Z, and Fu-Shan X
Br J Hosp Med (Lond) 2025; 86: 1-13
DOI: 10.12968/hmed.2024.0583
Abstract
Aims / Background
Dental anxiety (DA) often leads to significant fear and anxiety in the patients undergoing dental procedures, and increases the complexity and difficulty of treatment. Currently, remimazolam, a benzodiazepine-like sedative drug, has been found effective and safe during endoscopic and surgical procedures. Therefore, this study aimed to evaluate the safety levels and efficacy profile of remimazolam combined with remifentanil for sedation in adult patients with DA who underwent the mandibular impacted third molar extraction.
Methods
This single-center, retrospective cohort study included adult patients with DA who underwent mandibular impacted third molar extraction at the Beijing Stomatological Hospital between January 2021 and December 2023. Based on the sedation protocols used during dental procedures, patients were divided into two groups: a remimazolam combined with remifentanil group (the remimazolam group, n = 63) and a propofol combined with remifentanil group (the propofol group, n = 71). The overall incidence of adverse events was selected as the primary outcome measure, including pulse oxygen saturation (SpO2) <93%, injection pain, sedation failure, hypotension, bradycardia, and nausea/vomiting. The secondary outcome measures included sedation onset time, postoperative pain levels, satisfactions of patient and anesthesiologists, and vital signs changes over time.
Results
The remimazolam group showed an overall incidence of adverse events of 7.9%, compared to 49.3% in the propofol group, with a statistically significant difference between the two groups (p < 0.001). Both study groups demonstrated no statistically significant differences in sedation onset time (p = 0.252) and postoperative pain Verbal Rating Scale (VRS) score (p = 0.527). Moreover, the remimazolam group had greater stability in blood pressure (between-group effect, p = 0.012) and heart rate (between-group effect, p < 0.001) and exhibited statistically significant differences in changes in respiratory rate over time (between-group effect, p < 0.001).
Anesthesiologists’ satisfaction scores with respiratory and circulatory stability, sedation efficacy, and quality of sedation recovery were significantly higher in the remimazolam group compared to the propofol group (p < 0.001). Surgeons reported a higher satisfaction with sedation efficacy in the remimazolam group.
Conclusion
In summary, remimazolam combined with remifentanil demonstrates greater safety and effectiveness than propofol combined with remifentanil for sedation during dental procedures in adult DA patients. This combination particularly decreases adverse events, maintains stable respiratory and circulatory functions, and improves satisfaction levels among anesthesiologists and surgeons.
Reviewers evaluation, opinion and points of interest
This Chinese study compares a dual-drug regimen, remimazolam combined with remifentanil (n=63), against a propofol / remifentanil combination (n=71) for sedation during impacted mandibular third molar extraction in anxious adult patients. The key finding is compelling: the remimazolam group reported an adverse event incidence of only 7.9%, compared to a rate of 49.3% observed in the propofol group. This superior safety profile -with lower levels of hypotension and bradypnea - was achieved while maintaining an excellent quality of sedation as rated by the anaesthetist, the surgeon, and the patient.
Whilst the results are very encouraging, there were some methodological flaws. This was a single-centre, retrospective cohort study, which introduces potential selection and reporting biases compared to a prospective randomised controlled trial. However, the groups appear to have been comparable at baseline, and there was adequate standardisation of the surgical approach (impacted mandibular third molar extraction), lending weight to the findings.
The IACSD standards currently favour single-agent midazolam or remimazolam sedation, but there is significant demand for advanced techniques that offer more reliable sedation whilst maintaining a wide margin of safety. This data provides further support for remimazolam as a safe and efficacious sedative agent when combined with a fast-acting opioid (remifentanil).
GG
The 4P strategy for managing hypersensitive gag reflex: a case report and clinical guide
Kunasarapun P, Fisal A B A, IbnAhmad H, Phadraig C M G.
Spec Care Dentist 2025; 45: e70104
DOI: 10.1111/scd.70104
Introduction
The gag reflex is a protective physiological response that serves to prevent the entry of unwanted objects into the pharynx, larynx, and trachea through the involuntary contraction of oral and pharyngeal muscles [1]. It can be initiated by visual, auditory, olfactory, gustatory, mechanical, and psychological stimuli [2].
An exaggerated or hypersensitive gag reflex is an excessive motor reaction toward non-noxious stimuli affecting about 6%–8% of children and adults [3, 4]. A hypersensitive gag reflex can present extreme challenges for patients and dental professionals alike. Based on the authors’ experiences, this case report presents the use of the 4P Strategy for Managing Hypersensitive Gag Reflex. This represents the Preparatory, Psychological, Physical, and Pharmacological strategies that can be applied in combination to support patients who have a problem with gagging.
Reviewers evaluation, opinion and points of interest
Readers working in special care and anxious patient management will appreciate this thoughtful and practical paper, describing a structured approach to one of dentistry’s challenging clinical presentations - the hypersensitive gag reflex. In this detailed case report, the authors outline the ‘4P Strategy’, comprising Preparatory, Psychological, Physical and Pharmacological elements, to support patients for whom gagging has previously prevented care.
The paper presents an adult case study, with dyspraxia and generalised anxiety disorder, who had long avoided dental treatment due to a severe gag reflex. Endodontic care was successfully delivered through a carefully staged and collaborative plan; beginning with preparatory discussions that normalised gagging, setting realistic goals (‘to reduce, not eliminate’), and involving team rehearsal and clear patient control signals. Psychological strategies, including positive reinforcement, distraction, graded exposure and behavioural replacement techniques, were employed to reduce anxiety and interrupt the ‘gag–anxiety feedback loop’.
Physical adaptations were considered, including upright positioning, application of firm intraoral pressure, avoidance of trigger areas and extraoral radiography. These were combined with the pharmacological adjunct of nitrous oxide inhalation sedation (at 50% concentration). Dental treatment was completed successfully, reinforcing patient achievement and confidence in their ability to cope which, as I witness in my own clinical work, is fundamental in reducing negative cycles of reinforcement.
The authors’ 4P model provides a concise, memorable framework that integrates behavioural, physical and pharmacological strategies, underpinned by preparation, through strong communication and teamwork. While based on a single case, this paper offers a valuable clinical guide and reflective tool for practitioners; reminding us that effective management of the gag reflex is not merely technical, but psychological, relational and adaptive.
This paper is a highly readable and evidence-informed contribution, particularly useful for dental teams and behavioural clinicians supporting patients with complex sensory or anxiety-related responses to care.
JH
Examining barriers and facilitators of dental fear treatment adoption: A qualitative study of practicing dentists
Ochshorn J, Daly K A, Zaninovic V N, Heyman R E,
Smith Slep A M, Wolff M S.
PLoS One 2025; 20: e0322884
DOI: 10.1371/journal.pone.0322884
Abstract
Over fifteen percent of the global population experiences dental fear, and although evidence-based treatments exist, adoption of these treatments is almost non-existent. Informed by our prior research examining barriers to adopting face-to- face behavioral treatments in dental operatories, this study examined dentists' responses to three stepped-care Cognitive Behavioral Therapy for Dental Fear (CBT-DF) formats that use technology. All approaches offer an automated component as the first step (a mobile app) and either an in-person, virtual reality (VR), or video telehealth session as the second step. This study aims to understand which of these approaches would most likely be adopted by private practice dentists and why. Eight focus groups/solo interviews with a total of 13 private practice dentists were conducted with the aim to assess barriers and facilitators to implementing three stepped-care approaches of CBT-DF. The qualitative data obtained from these interviews was coded and analyzed according to Rogers' framework of innovation (relative advantage, compatibility, complexity, trialability, and observability). The results indicated that participants acknowledged the value of interventions to address dental fear, as they had personal experiences with fearful patients that impacted their practices. Participants responded positively to the automated component of treatment (the app) and were more wary of treatment options requiring office space and staff time (in-person VR and in- person mental health provider). The telehealth option received the most favorable response, although some doubts were expressed regarding relative efficacy and patient accountability. Thus, dissemination of an app-telehealth treatment model that allows dentists to serve as referral partners is promising, given dentists' incentives to decrease patient fear while avoiding opportunity cost (e.g. occupied chairs and staff time).
Reviewers evaluation, opinion and points of interest
This timely qualitative study addresses a question that my colleagues and I are often asked: ‘if Cognitive Behavioural Therapy for Dental Fear (CBT-DF) is so effective, why has it not been widely adopted in routine dental practice?’ Ochshorn and colleagues explored this through an implementation science lens, engaging 13 private practice dentists in focus groups and interviews to discuss three ‘stepped-care’ delivery models for CBT-DF; each combining a self-help app with either virtual reality exposure, telehealth or in-person delivery.
The authors analysed responses across key dimensions of relative advantage, compatibility, complexity, trialability and observability. While all participants recognised the clinical and financial impact of dental fear, enthusiasm for implementation depended on how easily interventions could fit within existing workflows. The app + telehealth model emerged as the most acceptable, allowing mental health professionals to deliver CBT remotely while dentists acted as referral partners; thereby reducing chair-time and disruption.
The findings also highlight a striking gap between dentistry and psychology; many dentists were unaware of the robust evidence base for CBT for dental anxiety, reflecting a broader need for education and dissemination through professional bodies, training programmes and digital platforms. Encouragingly, most participants valued the app component, seeing it as a practical screening and engagement tool.
The authors make a valuable contribution to this valuable research area of how to look to increase access to CBT in primary care settings, moving beyond efficacy to consider and address real-world feasibility of implementation. It reminds us that sustainable change in dental anxiety care will depend not only on the evidence-based treatments, but also on how well they are designed to integrate into the everyday realities of dental practice.
JH
Online cognitive-behavioural intervention to manage dental anxiety: a 12-month randomised clinical trial
Marisol Tellez M, Dunne E M, Konneker E, Zhao H, Ismail A I.
Community Dent Oral Epidemiol 2025; 53: 543–555
DOI: 10.1111/cdoe.13049
Abstract
Objective
The study aimed to test the efficacy of an online cognitive- behavioural therapy dental anxiety intervention (o-CBT) that could be easily implemented in dental healthcare settings.
Methods
An online cognitive-behavioural protocol based on psychoeducation, exposure to feared dental procedures and cognitive restructuring was developed. A randomised controlled trial was conducted (N = 499) to test its efficacy. Consenting adult dental patients (18-75 years old) who met inclusion criteria (e.g. high dental anxiety) were randomised to one of three arms, (a) intervention assisted by psychology staff (PI) (n = 162), (b) intervention assisted by dental staff (DI) (n = 167), or (c) a control condition (C) (n = 170). Primary outcome measures were the Modified Dental Anxiety Scale (MDAS) and the Anxiety and Related Disorders Interview Schedule DSM-V (ADIS) rating of fear. Generalised linear models for repeated measures based on intention to treat analyses were used to compare the three groups on dental anxiety, fear, avoidance and overall severity of dental phobia.
Results
Dental anxiety was significantly lower in both PI and DI groups when compared to the control condition. Interestingly, reductions in dental anxiety favoured the DI group at 6 (p = 0.008) and 12 months only (p = 0.009). Overall, equivalency was observed between the two intervention groups (PI and DI), as there were no significant differences in dental anxiety when the dental arm was compared to the psychology arm across all time points (p > 0.05).
Conclusion
The online cognitive-behavioural intervention was efficacious in reducing dental anxiety when compared to a control condition in an urban sample of patients receiving treatment in a dental school setting. Examination of its effectiveness when administered in dental offices under less controlled conditions is warranted.
Reviewers evaluation, opinion and points of interest
For those readers who follow this section of the Digest, you’ll know I often highlight innovations that aim to make evidence-based psychological care more accessible in dental settings. It also nicely supports the ideas outlined in the previous journal scan review. This paper by Téllez and colleagues reports on a recent large randomised controlled trial, testing an online cognitive behavioural therapy (o-CBT) programme for adults with dental anxiety.
Nearly 500 patients with high dental anxiety were randomised to one of three groups: (1) o-CBT assisted by psychology staff, (2) o-CBT assisted by dental staff, or (3) a control condition (a 1-hour nature video). The o-CBT intervention included education, motivational techniques, cognitive restructuring and graded video exposure to dental procedures; all delivered online, prior to a scheduled dental appointment.
The findings were really encouraging. Both o-CBT groups showed significant and lasting reductions in dental anxiety scores at 6 and 12 months, compared with controls. Importantly, outcomes did not differ between those supported by psychology or dental professionals, suggesting that this brief online intervention can be delivered effectively within dental settings by trained dental staff. While phobia severity and avoidance measures also improved, these changes did not reach statistical significance.
This study offers a strong case for scalable, non-pharmacological approaches to managing dental anxiety; approaches that could be integrated into existing care pathways without major disruption to practice flow. As the authors note, future work exploring multi-session or home- based versions could strengthen engagement and sustainability further.
This is a valuable and pragmatic piece of research that aligns well with the broader move towards digitally supported behavioural interventions in dentistry; and a sign of what accessible, psychologically informed care might look like in the future.
JH
The effectiveness of psychological interventions for the management of gagging among dental patients: a scoping review
O’Donald F, Smith M, Sevier-Guy L, Heffernan A.
Br Dent J 2025 Oct 17. Epub ahead of print.
DOI: 10.1038/s41415-025-8861-6
Abstract
Introduction
A sensitive gag reflex can significantly hinder patient dental care, and the optimal management strategy remains uncertain. Psychological interventions, such as systematic desensitisation, hypnotherapy, and relaxation techniques, have been explored as potential solutions. This scoping review aimed to evaluate the effectiveness of psychological interventions in managing the gag reflex in dental settings.
Methods
We systematically searched four electronic databases up to June 2024. Two reviewers screened and assessed articles, and relevant data were extracted on the delivery and outcomes of psychological interventions for managing gagging in dental settings.
Results
Eight studies involving 14 participants met the inclusion criteria. The psychological interventions examined included systematic desensitisation, hypnotherapy, and relaxation techniques, with an average intervention of five sessions over 19.3 weeks. All patients tolerated dental treatments post- intervention, and 87.5% reported an absence of gagging. No adverse effects were reported.
Conclusions
These findings suggest that psychological interventions hold promise in managing sensitive gag reflexes in dental patients. However, further research with standardised outcomes and larger sample sizes is needed to confirm their effectiveness. Additionally, further work is required to clarify when it is appropriate for dental staff to deliver these interventions themselves or refer patients to psychologists for specialised care.
Reviewers evaluation, opinion and points of interest
Following my other journal scan earlier highlighting the ‘4P Strategy’ (Preparatory, Psychological, Physical and Pharmacological) for gag reflex management, this scoping review draws together the evidence base underpinning the psychological components of such integrated approaches. I hope it will appeal to readers interested in the behavioural management of managing the gag reflex; a problem we know can severely disrupt dental care and often coexists with dental anxiety.
The authors systematically reviewed eight studies (14 patients in total) examining psychological approaches, including systematic desensitisation, hypnotherapy and applied relaxation, delivered over an average of five sessions across roughly 19 weeks. All patients went on to tolerate dental treatment following intervention and 87.5% reported no gagging during procedures.
While the evidence base remains small and limited to case reports, the consistency of successful treatment outcomes is notable. The review highlights that psychological approaches may be particularly effective where the gag reflex is maintained by associative learning, heightened anxiety or maladaptive (or unhelpful) beliefs; mechanisms familiar to those working within CBT frameworks for dental fear.
The methodological limitations are acknowledged, including a lack of standardised outcome measures, limited follow-up data, and variability in intervention delivery. The authors advocate for larger, well-designed studies using validated assessment tools to help establish when and how psychological techniques should be delivered, and by whom, within dental practice.
This clinically relevant review reinforces the importance of recognising gagging as both a physical and psychological phenomenon. It invites closer collaboration between dental teams and psychological professionals and provides a valuable synthesis of emerging evidence that could inform structured behavioural management strategies within dentistry.
JH